Family Support Data System Guide
This page was last updated on:
Introduction
Welcome to the Family Support Data System Guide. Please use the navigation on the right to jump to the relevant section of the page. All items can be expanded on the page using the Expand All Link above. Additional questions or suggestions can be emailed to the RA Account at: ra-pwpahomevisiting@pa.gov.
Overview of the Family Support Data System Guide Video
Please note this video was recorded in October 2021, there may have been changes to this page or additional features may be added that differ from the recording. Please feel free to email the RA Account above with any questions or clarifications.
Data System Forms
View Forms| Name | Downloads | Version | Last Modified | Download |
|---|---|---|---|---|
| Name | Downloads | Version | Last Modified | Download |
| 1065 downloads | 1.0 | 04-26-2022 14:19 | Download | |
| 618 downloads | 1.0 | 04-26-2022 14:19 | Download | |
| 615 downloads | 1.0 | 04-26-2022 14:19 | Download | |
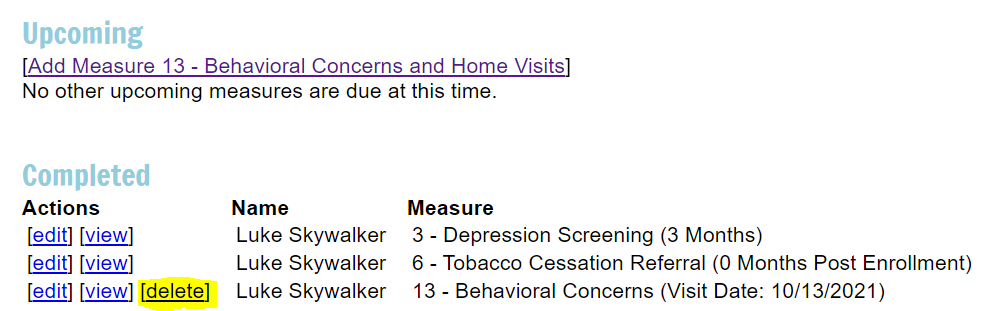
| 701 downloads | 1.0 | 04-26-2022 14:19 | Download | |
| 520 downloads | 2.0 | 08-04-2022 11:09 | Download | |
| 623 downloads | 1.0 | 04-26-2022 14:19 | Download | |
| 583 downloads | 1.0 | 04-26-2022 14:19 | Download | |
| 539 downloads | 1.0 | 04-26-2022 14:19 | Download | |
| 697 downloads | 1.0 | 04-26-2022 14:19 | Download | |
| 467 downloads | 2.0 | 02-07-2024 9:54 | Download | |
| 659 downloads | 1.0 | 04-26-2022 13:59 | Download | |
| 560 downloads | 1.0 | 04-26-2022 13:56 | Download | |
| 514 downloads | 1.0 | 04-26-2022 13:54 | Download | |
| 552 downloads | 1.1 | 04-26-2022 13:53 | Download | |
| 670 downloads | 1.0 | 04-26-2022 13:50 | Download | |
| 618 downloads | 1.0 | 04-26-2022 13:49 | Download | |
| 613 downloads | 1.0 | 04-26-2022 13:46 | Download | |
| 561 downloads | 1.0 | 04-26-2022 13:40 | Download | |
| 1908 downloads | 13 | 12-06-2023 13:12 | Download | |
| 705 downloads | 2.0 | 10-12-2021 8:28 | Download | |
| Name | Downloads | Version | Last Modified | Download | |
|---|---|---|---|---|---|
| Name | Downloads | Version | Last Modified | Download | |
| Data System Forms | |||||
| Data System Forms | |||||
| OLD - Understanding the PA Family Support Data Collection System | |||||
No files found in this folder. | |||||
Data Reports
View Reports| Name | Downloads | Version | Last Modified | Download |
|---|---|---|---|---|
| Name | Downloads | Version | Last Modified | Download |
| 749 downloads | 1.0 | 11-30-2021 11:14 | Download | |
| 620 downloads | 1.0 | 01-13-2021 8:58 | Download | |
| 700 downloads | 1.0 | 10-26-2020 10:19 | Download | |
| 812 downloads | 1.0 | 01-07-2019 10:29 | Download | |
| 813 downloads | 1.0 | 01-07-2019 10:29 | Download | |
| 734 downloads | 1.0 | 02-12-2018 10:12 | Download | |
| 726 downloads | 1.0 | 02-12-2018 10:12 | Download | |
| 855 downloads | 1.0 | 02-12-2018 10:11 | Download | |
How to Access the Pennsylvania Family Support Program Data System
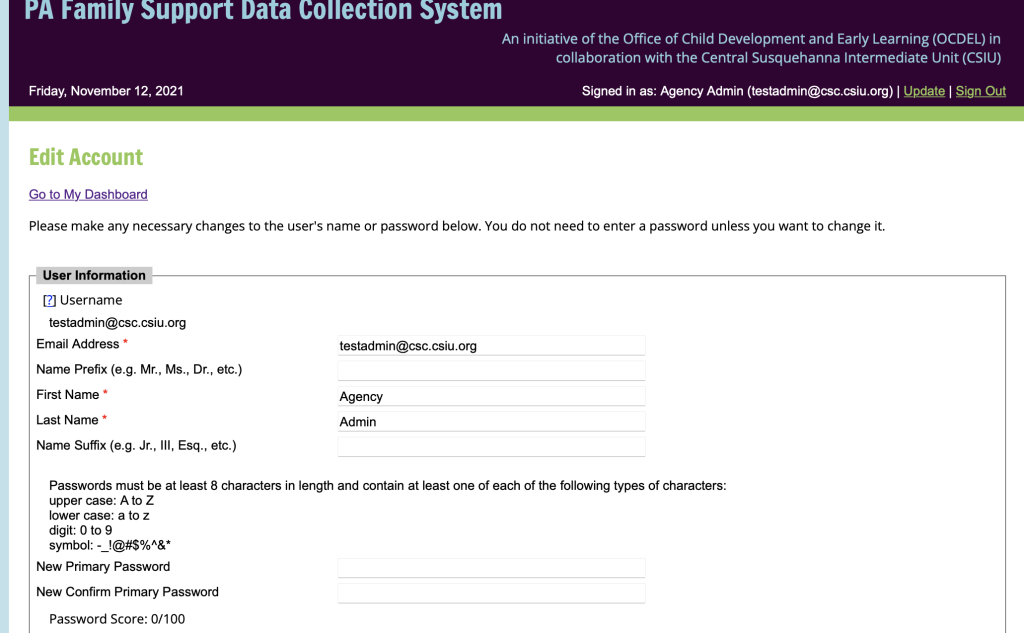
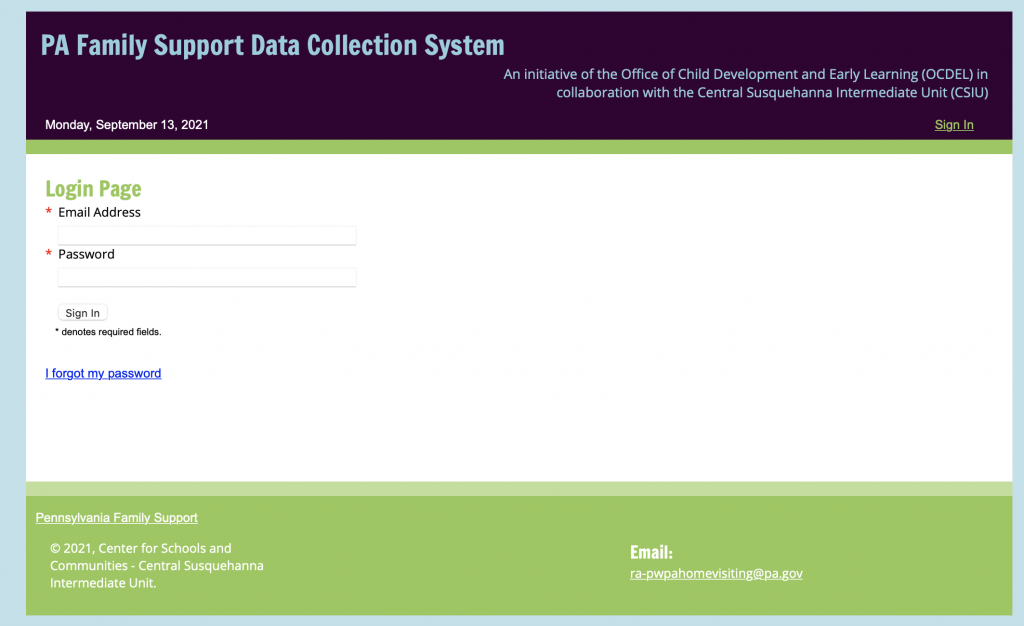
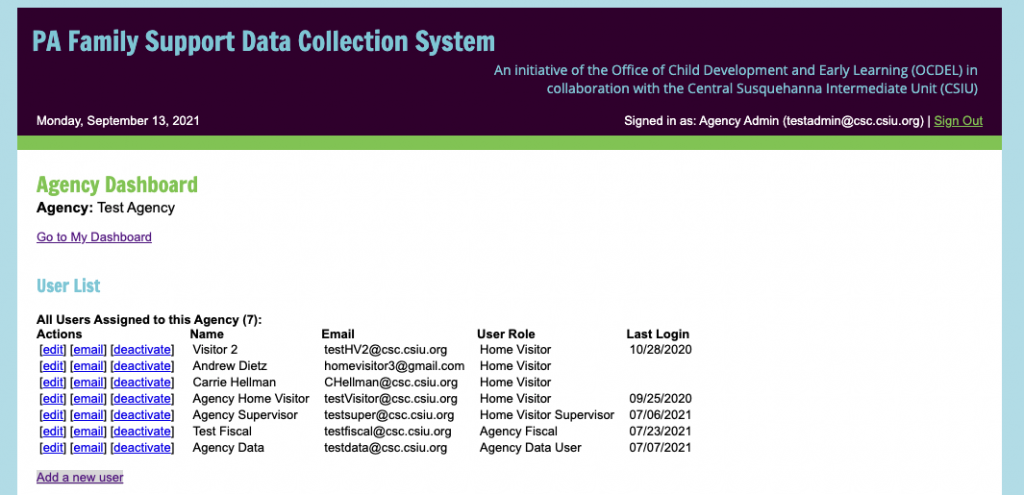
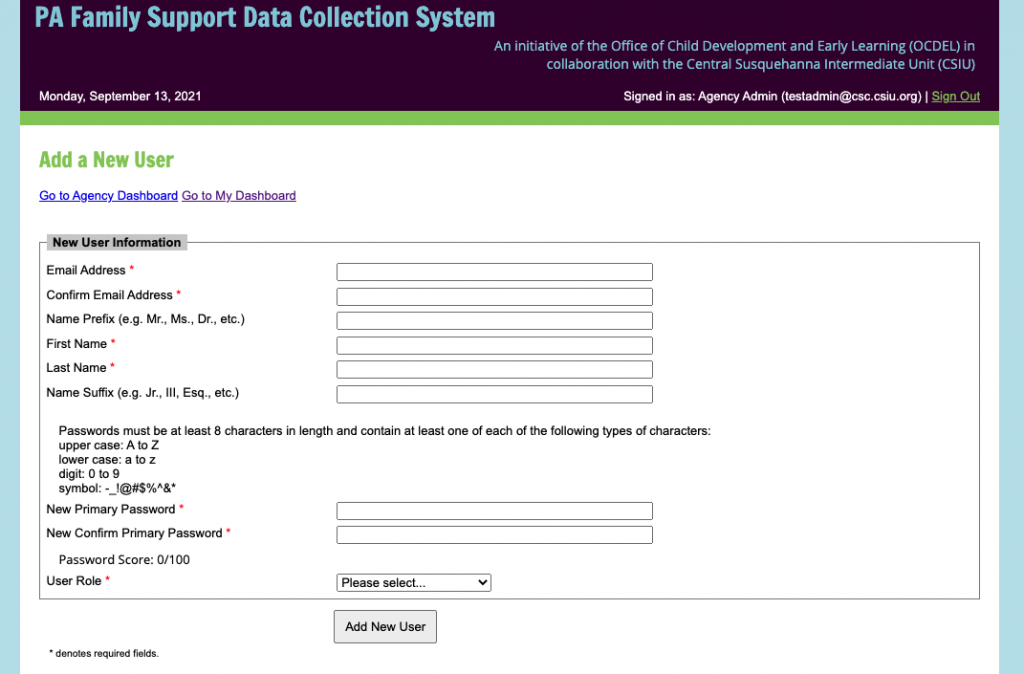
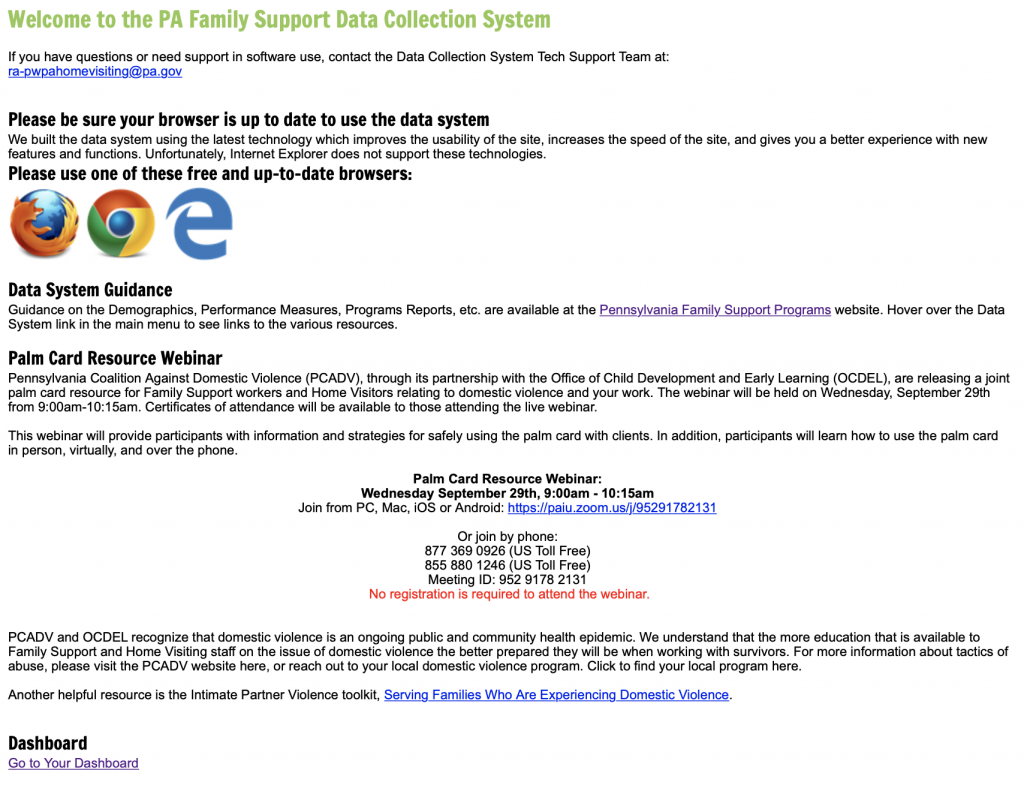
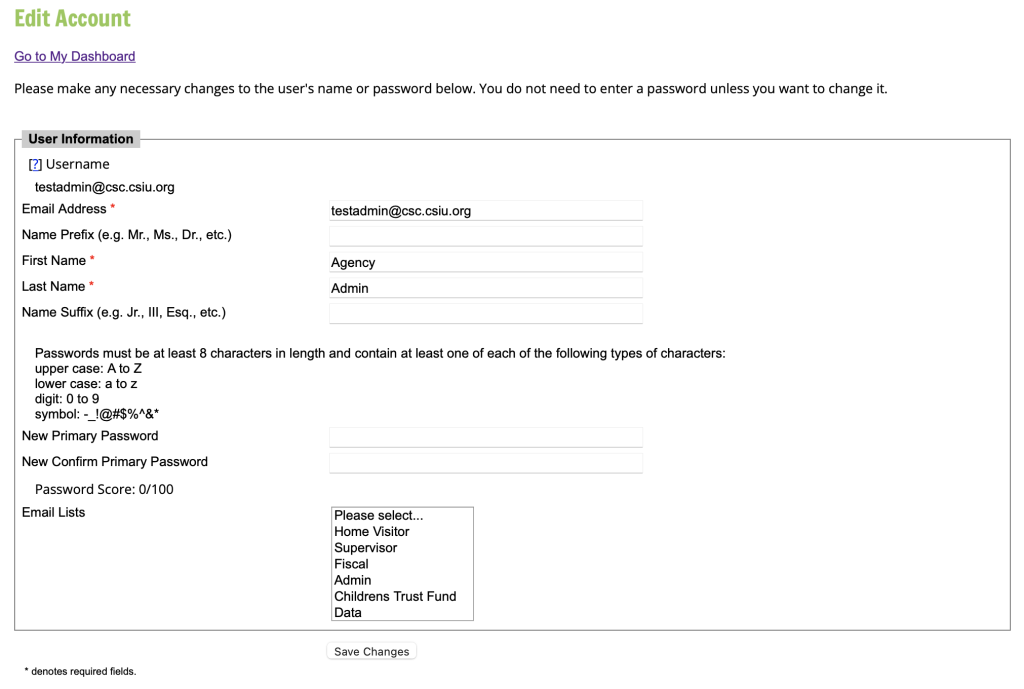
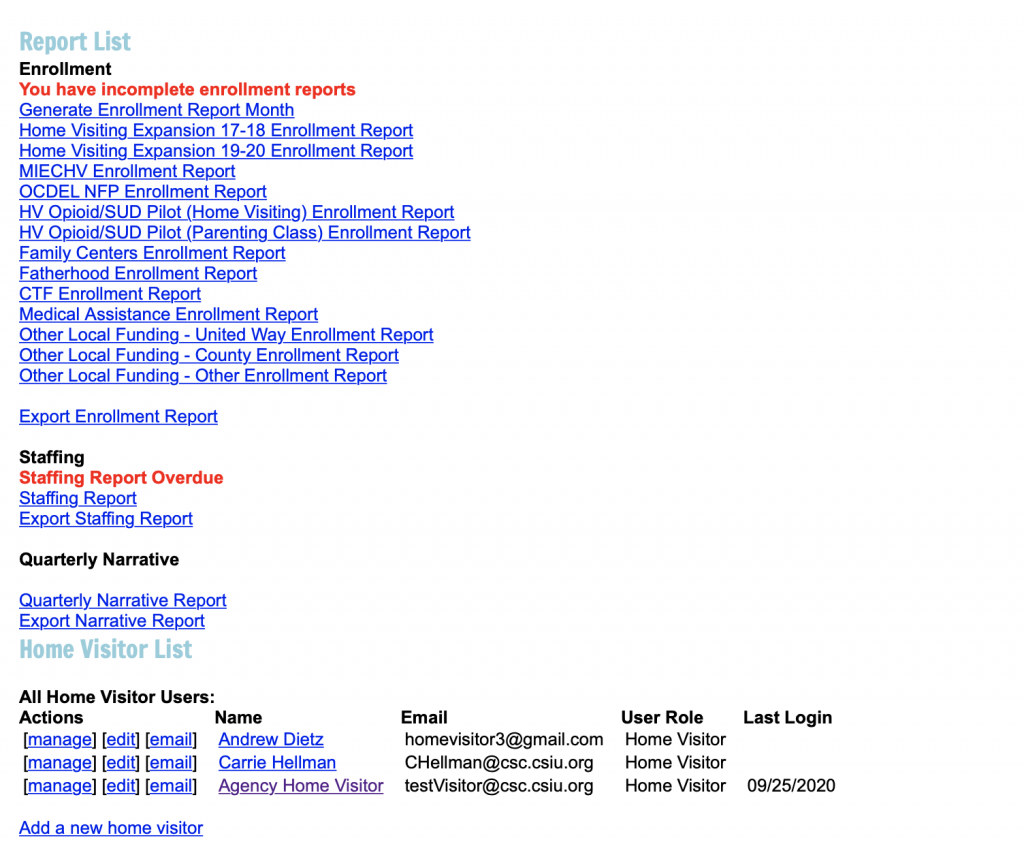
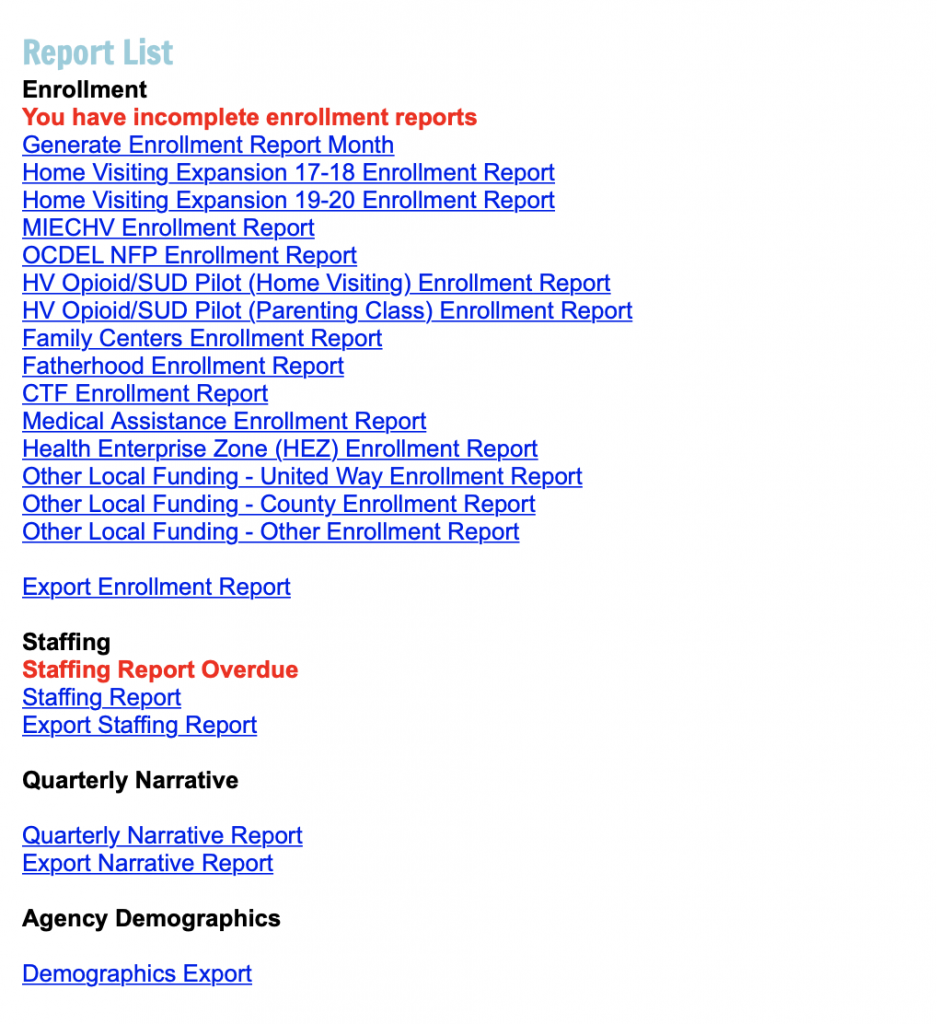
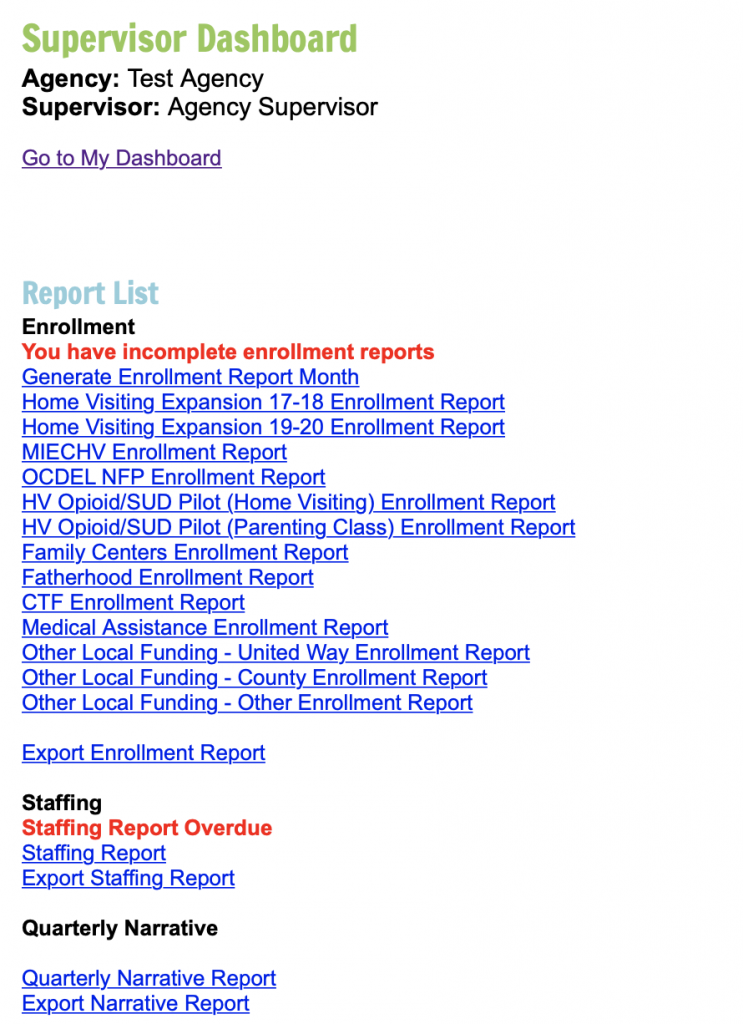
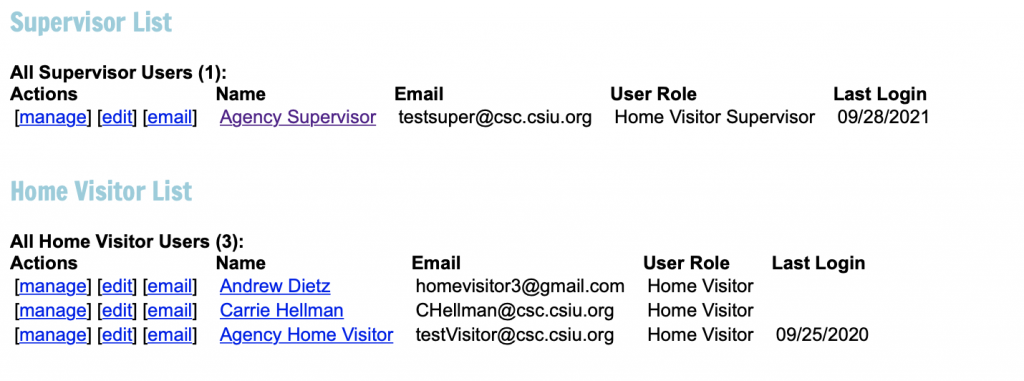
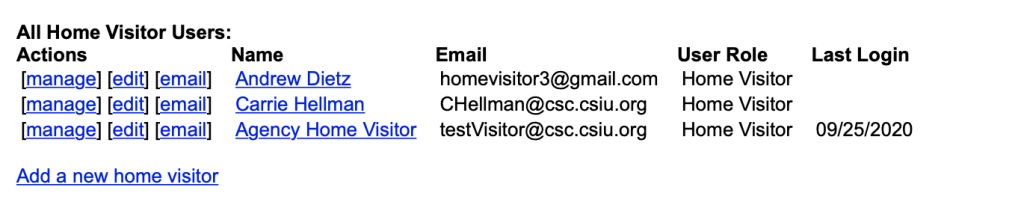
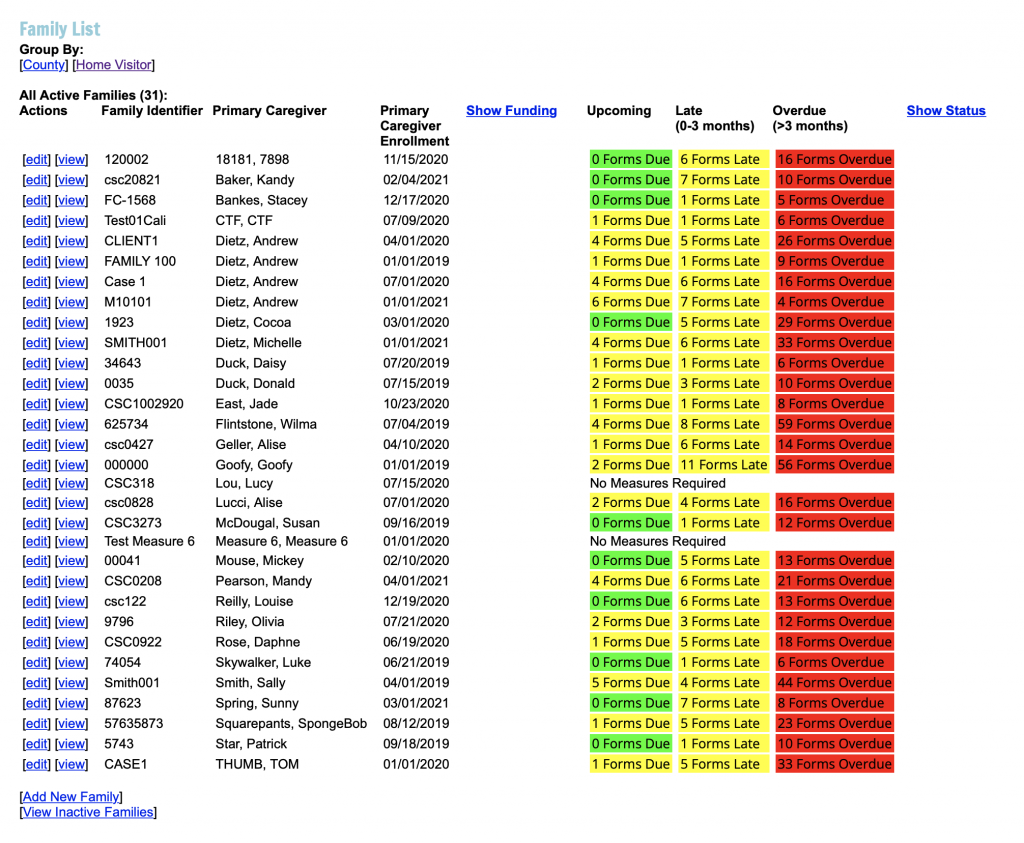
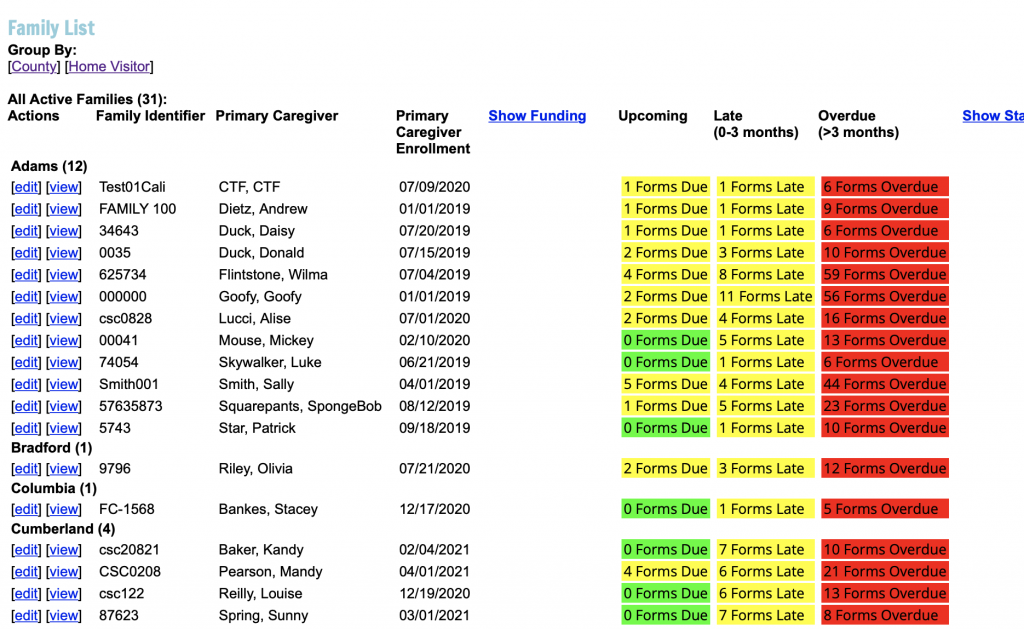
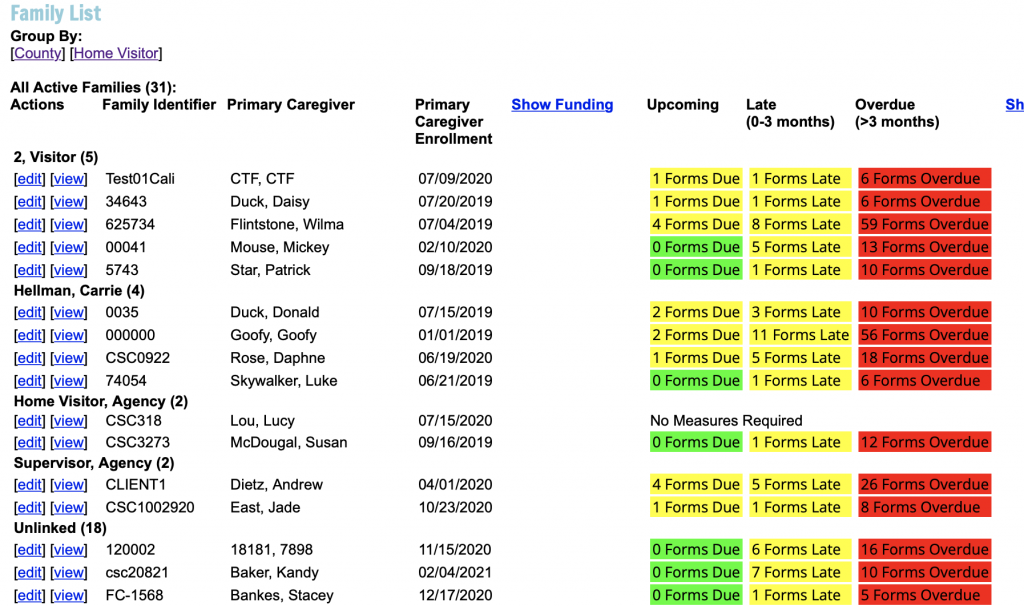
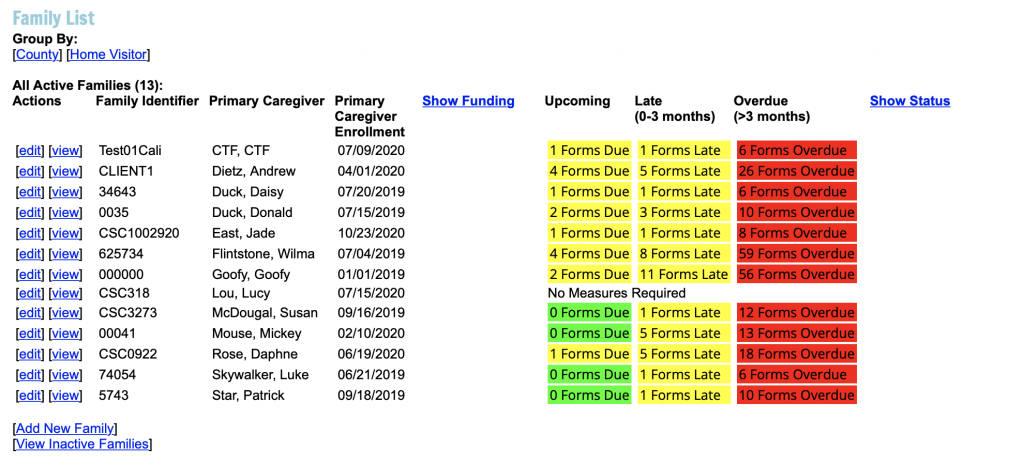
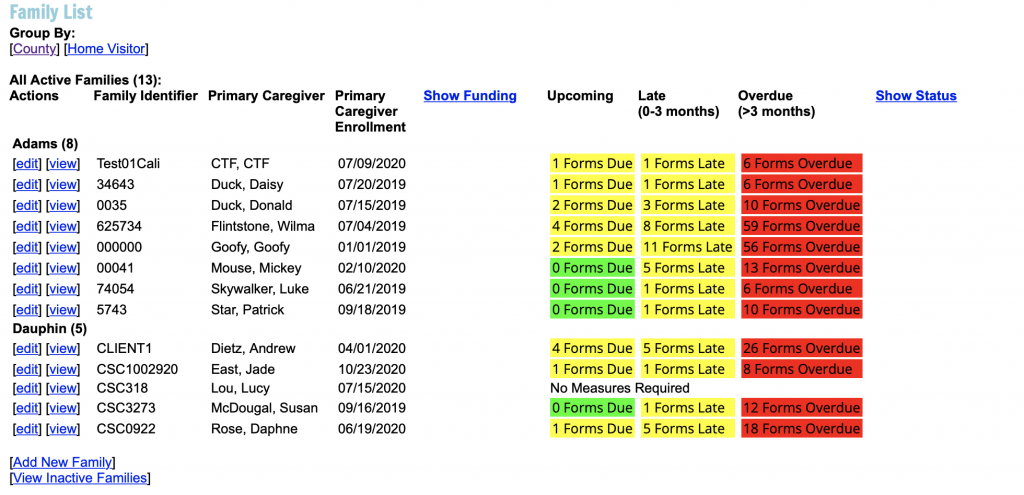
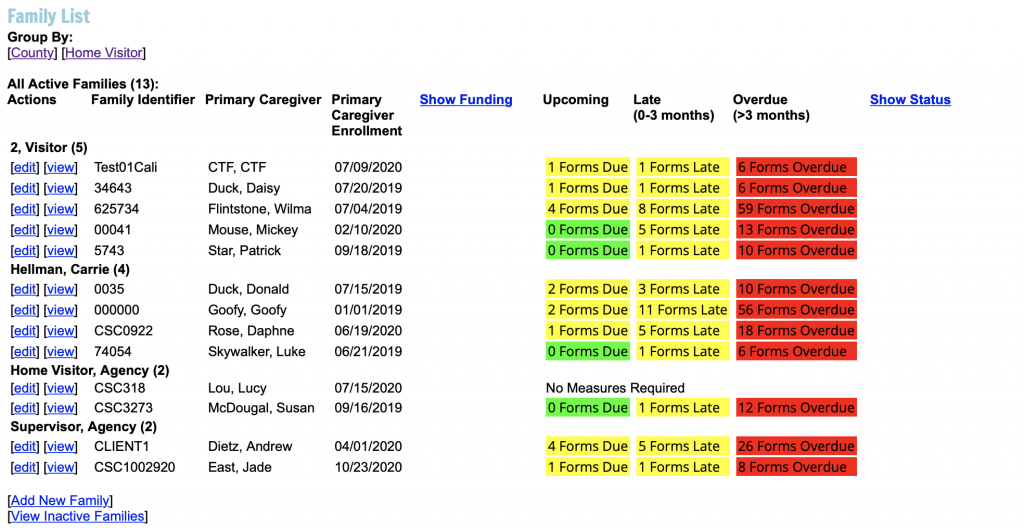
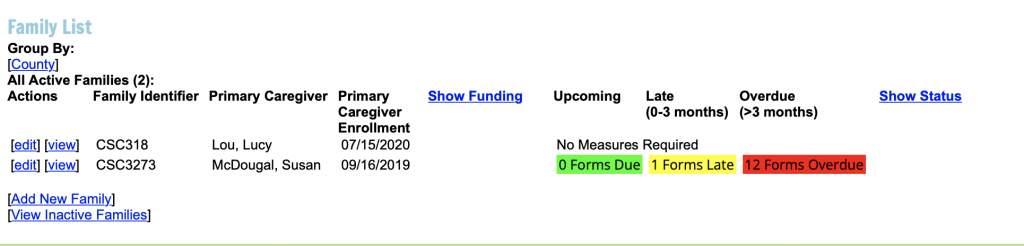
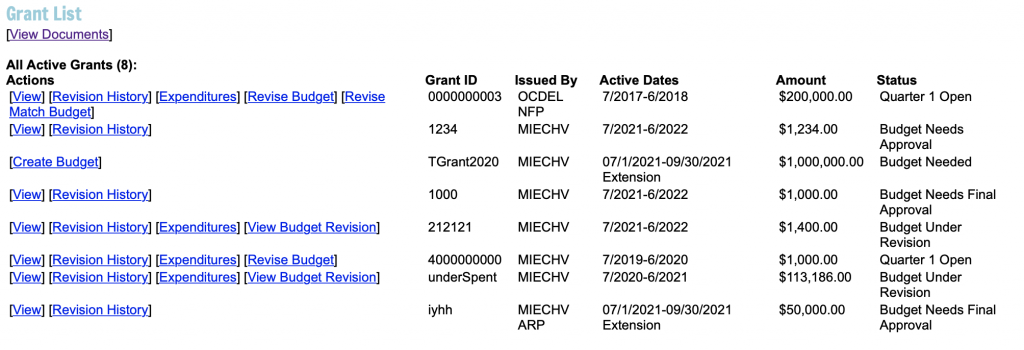
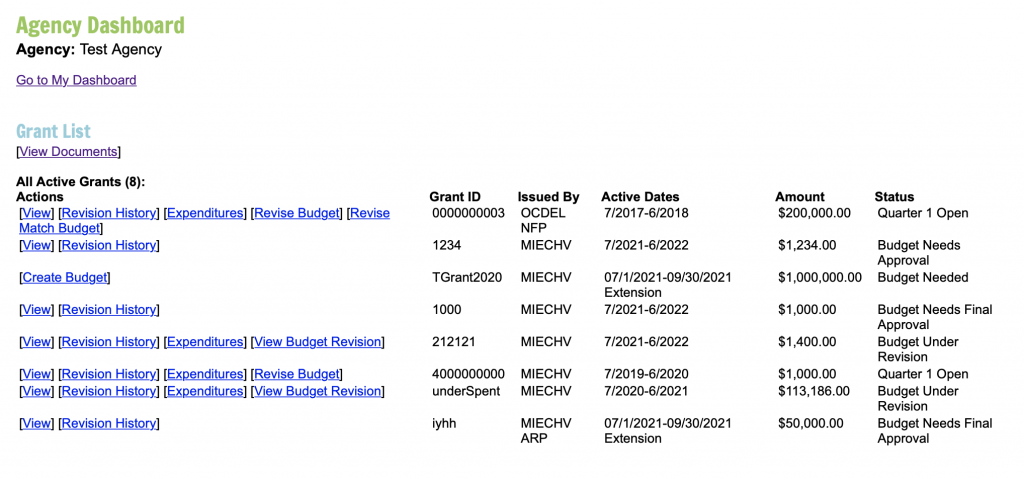
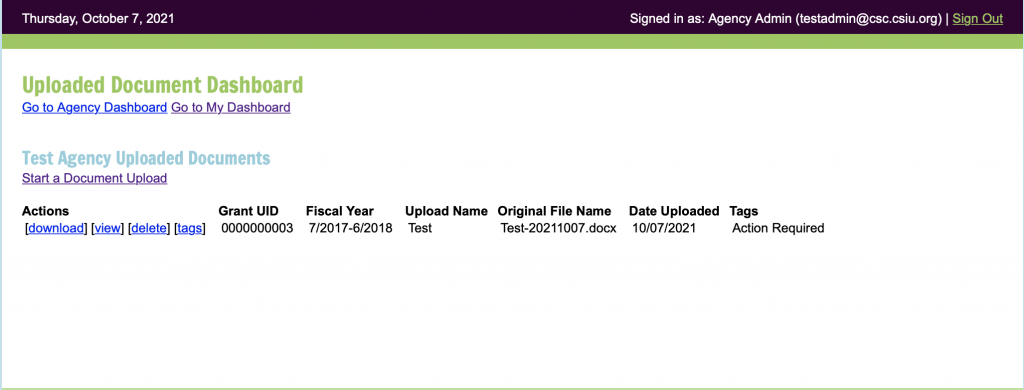
Video on how to Access the Pennsylvania Family Support Program Data System Update Password and Password Reset Update Password Step 1. Log in Step 2. Click Update next to sign out on the header Step 3: Update Password and other relevant information Forgot Password Step 1. Go to: https://data.pa-home-visiting.org/user/login. Step 2. Click the I forgot my password link at the bottom of the page. Step 3. Enter username (email address) and click Send Password Reset Email. Step 4: Look for an email (it might take a few mins and be sure to check your spam folder) and click the link in the email to reset the password. Step 5: If you do not receive an email please email the RA Account @ ra-pwpahomevisiting@pa.gov. User Types, Roles, and Permissions Home Visitor or Family Support Provider (Home Visitor in System) Home Visitor Supervisor or Family Support Supervisor (Home Visitor Supervisor in System) Agency Fiscal Agency Data User Agency Administrator Adding a New User After successfully logging into the system, depending on your User Level (see above) you will see different dashboards for those able to add users they will see a user list. Users will only see other users with user levels below their current level. Example: Agency Admins will not see Other Agency Admins listed at this time. Step 1. Click Add a new user. Step 2. Enter the required information for the user. Step 3. Enter a temporary password for that user. The user does not need to be provided with this password to perform a reset. See Step 6. Step 3a. When the new user logins for the first time they should request a password reset using the I forgot my password directions so that they can set a secure password they will remember. Step 4. Choose User Role (Level). See User Roles below. Step 5. Submit. Step 6. Let the user known to enter their email address into the I forgot my password screen so that they can reset their password. Dashboard Welcome Screen After successfully logging into the system this screen will display. This screen contains important information on using the data system, where to find data system guidance, and relevant training opportunities. Email Lists Email List Access Step 1. Log in Step 2. Click Update next to sign out on the header Step 3: Select Appropriate Email Lists, Control and Select to select multiple emails lists. Scroll down to see all lists available. Please definition of each email list type below. Email List Definitions Home Visitor -Should be selected if the person holds the Home Visitor User role in the data system. Supervisor -Should be selected if the person holds the Supervisor User role in the data system. Fiscal -Should be selected if the person holds the Fiscal User role in the data system. Should also be selected by Administrators that would like to be included on fiscal emails. Admin -Should be selected if the person holds the Admin User role in the data system. Children’s Trust Fund – Should only be selected if the Program currently holds a Children’s Trust Fund Grant. This will be used to provide emails specifically to any Children’s Trust Fund changes decided by the CTF Board. Data – Should be selected if the person holds the Data User role in the data system.Should also be selected by all users that would like to receive data system updates. CQI – Should be selected by appropriate users would like to receive emails related to Continuous Quality Improvement. Agency Reports – Should be selected by appropriate users to receive emails related to specific Agency Reports. Such as a data summary report. Program – Should be selected to by appropriate users that would like to receive programmatic updates note related to the data system. Please sign up for the data user list for data system updates. Video on Family Support Data System Dashboard Views User Lists Agency Administrator View The Agency Administrator will see all users. The Agency Admin will not see any other Agency Admins or themselves within the user list. The user list will be at the top of the Agency Dashboard after the welcome screen. User Deactivation Agency Data User View The Agency Data User will see all users except for Agency Administrators. The Agency Data User will not see any other Agency Data Users or themselves within the user list. The user list will be at the top of the Agency Dashboard after the welcome screen. User Deactivation Agency Supervisors View The Supervisor will see the home visitors they have been linked to by the Agency Administrator or Agency Data User. The Supervisor has the ability to add additional Home Visitors which will automatically be linked to them. The Supervisor will not see themselves or any additional Supervisors on a user list when they login to the system. The Home Visitor user list for the Supervisor role is located under the report section. Please see the image below. Agency Home Visitor and Agency Fiscal User The Home Visitor and Fiscal User Roles do not have access to the user lists. Report List Agency Administrator View The Agency Administrator has access to all reports. The reports are located below the User List on the Agency Dashboard. The designated user or users at the agency will complete the appropriate reports based on their funding for enrollment. All agencies will complete enrollment, staffing, quarterly narrative, the Agency Demographics Export and all future exports. Please note that additional reports and exports may be added in the future that differ from the image below. Agency Data User View The Agency Data User has access to all reports. The reports are located below the User List on their Agency Dashboard. The designated user or users at the agency will complete the appropriate reports based on their funding for enrollment. All agencies will complete enrollment, staffing, quarterly narrative, the Agency Demographics Export and all future exports. Please note that additional reports and exports may be added in the future that differ from the image below. Agency Supervisor View The Agency Supervisor has access to all reports. The reports are located at the top of their agency dashboard. The designated user or users at the agency will complete the appropriate reports based on their funding for enrollment. All agencies will complete enrollment, staffing, quarterly narrative. Please note that additional reports may be added in the future that differ from the image below. The Agency Supervisor does not have access to the demographic export at this time. Agency Home Visitor View The Agency Home Visitor role does not have access to the Report or Export List. Agency Fiscal View The Agency Fiscal User role does not have access to the Report or Export List. Supervisor List Agency Administrator View The Agency Administrator has access to the Home Visitor Supervisor List, located below the Report section on the dashboard. They can add new supervisors and link them to other Home Visitors using this list using the manage feature. Agency Data User View The Agency Data User has access to the Home Visitor Supervisor List, located below the Report section on the dashboard. They can add new supervisors and link them to Home Visitors using this list using the manage feature. Agency Supervisor View The Agency Supervisor Role does not have access to the Supervisor List Agency Home Visitor View The Agency Home Visitor Role does not have access to the Supervisor List Agency Fiscal View The Agency Fiscal Role does not have access to the Supervisor List Home Visitor List Agency Administrator View The Agency Administrator has access to the Home Visitor List, located below the Home Visitor Supervisor section on the dashboard. They can add new home visitors and link them to Home Visitors Supervisors and Families using this list using the manage feature. Agency Data User View The Agency Data User has access to the Home Visitor List, located below the Home Visitor Supervisor section on the dashboard. They can add new home visitors and link them to Home Visitors Supervisors and Families using this list using the manage feature. Agency Supervisor View The Agency Supervisor has access to the Home Visitors they added themselves as users or those they were linked to (by a Admin or Data User) using the manage feature. They can manage home visitors and link them to specific families if needed. Agency Home Visitor View The Agency Home Visitor Role does not have access to the Home Visitor List. Agency Fiscal View The Agency Fiscal Role does not have access to the Home Visitor List. Family List Agency Administrator View The Agency Administrator user role will see all families enrolled under the agency on the dashboard after logging in. They can sort the families by assigned Home Visitor (also includes Supervisor) and County. Sorted by County Sorted by Home Visitor Agency Data User View The Agency Data User role will see all families enrolled under the agency on the dashboard after logging in. They can sort the families by assigned Home Visitor (also includes Supervisor) and County. Sorted by County Sorted by Home Visitor Agency Supervisor View The Agency Supervisor User role will see all families linked to them or the home visitors they oversee (are linked to) within the Agency on the dashboard after logging in. They can sort the families by assigned Home Visitor (also includes Supervisor) and County. Sorted by County Sorted by Home Visitor Agency Home Visitor View The Home Visitor role will see the families they have entered themselves or that have been linked to them using the manage feature. The Home Visitors can sort by County if serving multiple counties. Sort by County Agency Fiscal View The Agency Fiscal user does not have access to the Family list. Inactive Families List Agency Administrator View The Agency Administrator role can access all “inactive” families. Inactive is defined as families that have exited the program either through completion or prior to completion or families that are currently on hold. The access for the Agency Administration is at the bottom of the family list. Agency Data User View The Data User role can access all “inactive” families. Inactive is defined as families that have exited the program either through completion or prior to completion or families that are currently on hold. The access for the Data User is at the bottom of the family list. Agency Supervisor View The Supervisor role can access “inactive” families that they directly entered or were linked to or that the home visitors they were linked to entered and placed into inactive status. Inactive is defined as families that have exited the program either through completion or prior to completion or families that are currently on hold. Agency Home Visitor View The Home Visitor role can access “inactive” families that they directly entered or were linked to. Inactive is defined as families that have exited the program either through completion or prior to completion or families that are currently on hold. The access for the Home Visitor is at the bottom of the family list. Agency Fiscal View The Agency Fiscal User does not have access to inactive families. Grant List Agency Administrator View The Agency Administrator User role has access to the Grant List. The list of all Grants assigned to the Agency is available at the bottom of the dashboard under the Family List. Agency Data User View The Agency Data User does not have access to the Grant list. Agency Supervisor View The Agency Supervisor User does not have access to the Grant list. Agency Home Visitor View The Agency Home Visitor User does not have access to the Grant list. Agency Fiscal View The Agency Fiscal User role has access to all Grants assigned to the Agency, when they login they will only see the Document Viewer link and Grant List at this time Document Viewer Directions on Uploading Agency Administrator View The Agency Administrator User role has access to the Document Viewer, the link to view, download, upload and delete documents is available below the Family List as a link under the Grant List Header. To Upload a Document: Click the start a Document Upload Link and the following screen will display. To upload a document you will need to select the grant in which it applies, we will be adding an option for Not Applicable soon. Agency Data User View The Agency Data User does not have access to the Document Viewer Agency Supervisor View The Agency Supervisor User does not have access to the Document Viewer Agency Home Visitor View The Agency Home Visitor User does not have access to the Document Viewer Agency Fiscal View The Agency Fiscal User role has access to the Document Viewer but using the View Documents link under the Grant List header. To Upload a Document: Click the start a Document Upload Link and the following screen will display. To upload a document you will need to select the grant in which it applies, we will be adding an option for Not Applicable soon. Entering a Family Caregiver and Child For definitions please see below. Updating a Family Caregiver and Child Updating a Family, Caregiver, and Child Funding Type Exiting and Un-exiting a Family Caregiver and Child For definitions please see below. Placing a Family on Hold For definitions please see below. Transferring Families Between Agencies If a known Family was enrolled in the same EBHV at another agency funded by OCDEL, their information can be transferred from the prior agency to the new agency. Linking Users to Staff and Families For definitions please see below. Removing Accidental Family and Measure 13 Entries Removing Accidental Families Step 1: If multiple families have been created that do not have any demographics entered they can be deleted by the home visitor or any user type except fiscal off of the family list. Step 2: Click on View next to the Family and the Delete Option will be present. Step 3: Select Yes to Confirm Deletion or No to keep the family. Step 4: If demographics have been entered an Agency Administrator or Data User can delete the Families, they must first delete any children added, followed by caregivers, and then finally the family. For definitions please see below. Removing Measure 13 Deletion – Behavioral Concerns and Number of Home Visits Step 1: View completed measures list at the bottom of a family dashboard. Step 2: Select delete next to an entered Measure 13. Step 3: Select Yes to confirm deletion or no to keep the measure as is. Family Demographics (Household) Collected *Family (Case) Identifier – A unique number that identifies the family in the data system. Some agencies choose to use a code for funding, others match their model data system identifiers. This is defined by the Agency there is no specific requirements from OCDEL on which identifier to use, however each Family must have a unique identifier. *Total number of people in the household – The household may include multiple adult caregivers (e.g., pregnant women, female caregiver, male caregiver). The number should include all participants in the program, plus anyone else living in the home who provides financial support to the participant(s). *Annual Household Income – Household income refers to the annual gross income for the household, and recorded at enrollment and then annually thereafter. NFP Income Crosswalk *Users of tobacco products – Based on self-report, a household with members who use tobacco products in the home or who have been identified as using tobacco through a substance abuse screening administered during intake. *Have low student achievement (any Caregiver and/or child in the home) – Based on self-report, a household with members who have perceived themselves or their child(ren) as having low student achievement. When answering this question, consider anyone who is living in the home. Please note that these answers will not be compared to the answer for “Number of People in Household”. *Have a child with developmental delays or disabilities (any child in home) – Based on self-report or home visitor/staff observation, a household with members who have a child or children suspected of having a developmental delay or disability. When answering this question, consider anyone who is living in the home. Please note that these answers will not be compared to the answer for “Number of People in Household”. *Family member is serving, or formerly served, in the US armed forces (any family member living in the home) – Based on self-report, households that include individuals who are currently serving or formerly served in the Armed Forces, including such households that have members of the Armed Forces who have had multiple deployments outside of the United States. This definition includes a military member’s dependents, which includes dependents acquired through marriage, adoption, or other action during the course of a member’s current tour of assigned duty. When answering this question, consider anyone who is living in the home. Please note that these answers will not be compared to the answer for “Number of People in Household”. *Household has a history of child abuse or neglect or has had interactions with child welfare services (any Caregiver and/or child in the home) – Based on self-report, a household with members who have a history of abuse or neglect and have had involvement with child welfare services. This can include the child, adult caregivers, or both. When answering this question, consider anyone who is living in the home. Please note that these answers will not be compared to the answer for “Number of People in Household”. *Primary Referral Source – Based on self-report or information provided to the Family Support Program for the referral. Caregiver Demographics Enrollment Collected *First Name – First name of the Client (Caregiver) Middle Name – Middle name of the Client (Caregiver) if applicable *Last Name – Last name of the Client (Caregiver) *Caregiver (Client) Identifier – A unique number to identify the Caregiver in the data system. Some agencies choose to use a code for funding, others match their model data system identifiers. *Family (Case) Identifier – A unique number that identifies the family in the data system. Some agencies choose to use a code for funding, others match their model data system identifiers. *Evidence-Based Home Visiting (EBHV) Program – An approved EBHV on the HomeVEE list of EBHV programs *Family Support Programs – All other programs not on the HomVEE list supported by state and federal funding sources through the Grants Contracts provided by OCDEL. *Program Type (Funding) – The funding being used to support the Family. Staff that support the families are usually designated to a funding stream or if split a certain percentage of their families are designated to that funding. Example: If a Home Visitor is 50% MIECHV and 50% Family Center (FC) with a Caseload of 20 families, usually 10 will be assigned to MIECHV funding and 10 will be assigned to FC funding. *Date of Enrollment – The date the Caregiver enrolled in either the EBHV or Family Support Program or both. Demographics Collected *Caregiver Identifier – A unique number to identify the caregiver in the data system. Some agencies choose to use a code for funding, others match their model data system identifiers. *Address – Caregiver’s housing unit address that has a house number and street name address, for example, 212 Elm Street or 137 Clark Ct., Apt. 316, as city-style addresses. In some instances, the house number may also include an alpha character such as 35A or W9254. The addresses that is used for mailing or to provide location for emergency services, such as police, fire, and rescue (E-911 addresses). Includes the County in which the Caregiver resides. *Birth Date – The official month, day, and year a caregiver was born. *Gender – (Effective 10/1/2021) *Pregnancy Status – Is the caregiver pregnant, or not pregnant. Pregnancy: The state of carrying a developing embryo or fetus within the body. This condition can be indicated by positive results on an over-the-counter urine test, and confirmed through a blood test, ultrasound, detection of fetal heartbeat, or an X-ray. *Estimated Date of Delivery – The estimated date of delivery, also known as expected date of confinement, and estimated due date or simply due date, is a term describing the estimated delivery date for a pregnant person. *History of Substance Abuse – Caregiver has a history of substance abuse, but is not currently abusing substances. Substance abuse, also known as drug abuse, is a patterned use of a drug in which the user consumes the substance in amounts or with methods which are harmful to themselves or others, and is a form of substance-related disorders. Including, but not limited to, illicit or street drugs (including, but not limited to, Alcohol, Bath salts, Cocaine, Crack, Ecstasy, Heroin, Inhalants, Ketamine, Marijuana, and Meth) and prescription drugs (including, but not limited to, Adderall, Ambien, Ativan, Hydrocodone, Oxycodone, Percocet, Tramadol, Valium, Vicodin, Vyvanse, and Xanax). *Current Substance Use / Needs Substance Abuse Treatment -Caregiver is currently struggling with substance abuse, and is actively or not actively receiving services for addiction or abuse. Substance abuse, also known as drug abuse, is a patterned use of a drug in which the user consumes the substance in amounts or with methods which are harmful to themselves or others, and is a form of substance-related disorders. Including, but not limited to, illicit or street drugs (including, but not limited to, Alcohol, Bath salts, Cocaine, Crack, Ecstasy, Heroin, Inhalants, Ketamine, Marijuana, and Meth) and prescription drugs (including, but not limited to, Adderall, Ambien, Ativan, Hydrocodone, Oxycodone, Percocet, Tramadol, Valium, Vicodin, Vyvanse, and Xanax). *Self-Identified Disability (Required 4/1/2021) – The definition of a person with disability has the same meaning for a child or adult with disability under the Individuals with Disabilities Education Act (IDEA) Parts B and C. *Plans of Safe Care – List and directs services and supports to ensure the safety and well-being of a substance-affected infant (SAI) and their caregivers. Plans of Safe Care differ from other safety or family service plans by including services for the infant and their substance affected caregiver(s). *Race – A Caregiver’s response to the race question is based upon self-identification. The responses regarding race should reflect what the person considers themselves to be and are not based on percentages of ancestry. Participants who select more than one race should be reported in the “Multiple Races” category. *Ethnicity – The responses regarding ethnicity should reflect what the person considers themselves to be and are not based on percentages of ancestry. *Legal Martial Status – The legal marital status refers to the marital status of a person under the law. *Educational Attainment – Educational attainment is defined as the highest grade completed within the most advanced level attended in the educational system of the country where the education was received. *Educational Status – Educational attainment or level of education of individuals. Current status of caregiver’s enrollment in school or training/certification courses. *Employment Status – Full-time employment is defined as working an average of 30 or more hours per week. Part-time is defined as working less than an average of 30 hours per week. A worker may be a full-time employee, part-time employee, or an employee on a casual basis. Caregiver could be employed temporarily, or on a permanent basis. *Housing Status – Status defined as the legal situation of household concerning the caregiver’s occupancy of their main residence. Caregiver is not homeless or homeless. *Health Insurance Status – Health insurance is a means for financing a caregiver’s health care expenses. Private health insurance as a plan provided through an employer or a union and coverage purchased directly by an individual from an insurance company or through an exchange (i.e. Aetna, Blue Cross). Government insurance coverage includes federal programs, such as Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), individual state health plans, TRICARE, CHAMPVA (Civilian Health and Medical Program of the Department of Veterans Affairs), as well as care provided by the Department of Veterans Affairs and the military. Caregiver’s are uninsured if they are not covered by any type of health insurance. *Measure 15: Caregiver Education (Only on Update) – This Measure will only display when updating if the Caregiver does not have a High School Diploma or Equivalent such as a GED. Child Demographics Collected *Child Identifier – A unique number to identify the child in the data system. Some agencies choose to use a code for funding, others match their model data system identifiers. *Gender – (Updated 05/01/2023) *Birth Date – The official month, day, and year a child was born. *Enrollment – Enrollment date cannot be before child’s birth date. Models are not chosen for the child as they are collected on the Caregivers Demographic screen. *Caregiver’s Relationship to Child – Refers to the unique and enduring bond between a caregiver and the child. Caregiver status in relation to biological, adoptive, or other caregiver status. *Caregivers Pregnancy Status – Only displays if the Caregiver is entered as pregnant. When entering the child it displays (due to the possibility of caregivers having multiple children). *Child’s Birth Weight – Birth weight is the body weight of the baby at its birth. Pounds (lbs) and ounces (oz.) *Child’s Gestational Age at Birth – Gestational age is the common term used during pregnancy to describe how far along the pregnancy is. Gestational Age at Birth is given in weeks and days. It is measured in weeks, from the first day of the woman’s last menstrual cycle to the current date. Since the exact date of conception is almost never known, the first day of the last menstrual period is used to measure how old the baby is. *Born Affected by Prenatal Substance Exposure / Plans of Safe Care – Relates to updates to the Child Protective Services Law. If a child was born substance exposed a plan of safe care is required to be developed for the infant and their family. “Affected by” is defined as an “infant with detectable physical, developmental, cognitive, or emotional delay or harm that is associated with maternal substance use or withdrawal, as assessed by a health care provider. http://www.keepkidssafe.pa.gov/cs/groups/webcontent/documents/document/c_292112.pdf *Race – A Caregiver’s response to the race question is based upon self-identification for their child. The responses regarding race should reflect what the person considers their child to be and are not based on percentages of ancestry. Participants who select more than one race for their child should be reported in the “Multiple Races” category. *Ethnicity – The responses regarding ethnicity should reflect what the person considers their child to be and are not based on percentages of ancestry. *Primary Language Spoken at Home – Primary Language spoken at home to the child. *Self-Identified Disability (Required 4/1/2021) – The federal definition of Disability for this data collection point is as follows: The definition of a person with disability has the same meaning for a child or adult with disability under the Individuals with Disabilities Education Act (IDEA) Parts B and C. *Health Insurance Status – Health insurance is a means for financing a child’s health care expenses. Private health insurance as a plan provided through an employer or a union and coverage purchased directly by an individual from an insurance company or through an exchange (i.e. Aetna, Blue Cross). Government insurance coverage includes federal programs, such as Medicare, Medicaid, the Children’s Health Insurance Program (CHIP), individual state health plans, TRICARE, CHAMPVA (Civilian Health and Medical Program of the Department of Veterans Affairs), as well as care provided by the Department of Veterans Affairs and the military. Caregiver’s are uninsured if they are not covered by any type of health insurance. *Usual Source of Medical Care – Usual source of care is the particular medical professional, doctor’s office, clinic, health center, or other place where a caregiver would usually go or bring their child to or contact if the child is sick, for well-visits or check-ups, or in need of advice about their health. *Usual Source of Dental Care – Usual source of care is the particular medical professional, doctor or dentist, clinic, health center, or other place where a caregiver would usually bring their child to or contact for oral or dentistry concerns, for well-visits or check-ups, or in need of advice about their health. Benchmark Areas Measure 1: Preterm Birth Definition: Percent of infants (among Caregivers who enrolled in home visiting prenatally before 37 weeks) who are born preterm following program enrollment. Caregiver Measure. M1 Preterm Birth FAQ's When is this collected? How is Preterm Birth Defined for this measure? How is this calculated for reporting purposes? Reporting Period Clarification: Measure 2: Breastfeeding Definition: Percent of infants (among mothers who enrolled in home visiting prenatally) who were breastfed any amount at 3 and 6 months of age. Caregiver Measure. M2 Breastfeeding FAQ's When is this collected? How is this calculated for reporting purposes? How is medical issue defined? Q) Does feeding a child pumped breast milk count as breastfeeding? Measure 3: Depression Screening Definition: Percent of primary caregivers enrolled in home visiting who are screened for depression using a validated tool within 3 months of enrollment (for those not enrolled prenatally) or within 3 months of delivery (for those enrolled prenatally). Caregiver Measure. Validated Screening Tools Please note as of 10/1/21 The Patient Health Questionnaire-2 (PHQ-2) and the Center for Epidemiological Studies Depression Scale Revised (CESD-R) are no longer consider validated tools for the purpose of this data collection. Brief Depression Inventory- II (BDI-II) Brief Symptom Inventory (BSI) Center for Epidemiological Studies Depression Scales (CES-D) Composite International Diagnostic Inventories (CIDI) – Short Form- Major Depression, Generalized Anxiety Disorder, Alcohol Dependence, Drug Dependence Depression Anxiety Stress Scales (DASS) Edinburgh Postnatal Depression Scale (EPDS) 10-item non-standardized self-report measure assessing maternal postnatal/postpartum depression. Patient Health Questionnaire-9 (PHQ-9) Postpartum Depression Screening Scale TM (PDSSTM) Zung Self-Rating Depression Scale M3 Depression Screening FAQ's When is this collected? How is this calculated for reporting purposes? Q) Do we screen primary caregivers who are already receiving services? Q) What is the considered a positive score if using the PHQ-9 as a screening tool? Measure 4: Well Child Visit Definition: Percent of children enrolled in home visiting who received the last recommended visit based on the American Academy of Pediatrics (AAP) schedule. Child Measure. M4 Well Child Visit FAQ's When is this collected? How is this calculated for reporting purposes? Q) Do we select only the one the client attended in the last 3 months or all visits? Q) When a child is older, do they need to attend a well-child visit every 3 months? Q) Is this Caregiver self-reported or do we need documentation? Q) Do Tele-Health Visits count for this measure? Measure 5: Postpartum Care Definition: Percent of Caregivers enrolled in home visiting prenatally or within 30 days after delivery who received a postpartum visit with a healthcare provider within 8 weeks (56 days) of delivery. Caregiver Measure. M5 Postpartum Care FAQ's When is this collected? How is this calculated for reporting purposes? Q) What is a postpartum visit? Q) Do Tele-Health Visits count for this measure? Measure 6: Tobacco Cessation Definition: Percent of primary caregivers enrolled in home visiting who reported using tobacco or cigarettes at enrollment and were referred to tobacco cessation counseling or services within 3 months of enrollment. Caregiver Measure. M6 Tobacco Screening Referrals FAQ's When is this collected? How is this calculated for reporting purposes? Q) How is other forms of nicotine defined? Q) What are Examples of tobacco cessation counseling or services? Q) What counts are providing a referral, what if the client declines? Measure 7: Safe Sleep Definition: Percent of infants enrolled in home visiting that are always placed to sleep on their backs, without bed-sharing or soft bedding. Child Measure. M7 Safe Sleep FAQ's When is this collected? How is this calculated for reporting purposes? Q) If not practicing safe sleep practices is the expectation to provide resources? Q) If the mother falls asleep with her infant after breastfeeding. How do you respond? Q) What are Examples of soft bedding? Measure 8: Child Injury Definition: Rate of injury-related visits to the Emergency Department (ED) since enrollment among children enrolled in home visiting. Child Measure. M8 Child Injury FAQ's When is this collected? How is this calculated for reporting purposes? Q) How is injury defined? Q) Is ingestion considered an injury? Measure 9: Child Maltreatment Definition: Percent of children enrolled in home visiting with at least 1 investigated case of maltreatment following enrollment within the reporting period. Child Measure. M9 Child Maltreatment FAQ's When is this collected? How is this calculated for reporting purposes? Measure 10: Parent-Child Interaction Definition: Percent of primary caregivers enrolled in home visiting who receive an observation of caregiver-child interaction by the home visitor using a validated tool. Child Measure. Validated Screening Tools CHEERS Check-In Dyadic Assessment of Naturalistic Caregiver- Child Experiences Emotional Availability Scale (EAS) – Added 10/1/2021 Home Observation for the Measurement of the Environment Keys to Interactive Parenting Scale PCI Feeding and Teaching Scales (formerly NCAST Nursing Child Assessment Feeding Scale and NCAST Nursing Child Assessment Teaching Scale) – Added 10/1/2021 Parenting Interactions with Children (Checklist of Obser-vations Linked to Outcomes (PICCOLO™) M10 Parent-Child Interaction FAQ's When is this collected? How is this calculated for reporting purposes? Q) What if the child is too young or too old for our chosen tool? Measure 11: Early Language and Literacy Definition: Percent of children enrolled in home visiting with a family member who reported that during a typical week s/he read, told stories, and/or sang songs with their child daily, every day. Child Measure. M11 Early Language and Literacy FAQ's When is this collected? How is this calculated for reporting purposes? Q) How should the question be answered if the Caregiver shares or loses custody? Q) What should be entered if other Family Members are reading, telling stories, or signing songs to the Child? Measure 12: Developmental Screening Definition: Percent of children enrolled in home visiting with a timely screen for developmental delays using a validated parent-completed tool. Child Measure. Validated Screening Tools Ages and Stages Questionnaires, 3rd Edition (ASQ-3) M12 Developmental Screening FAQ's When is this collected? How is this calculated for reporting purposes? Q) My model(s) screening times does not align with the AAP recommendations? Q) What about the ASQ: Social-Emotional (ASQ: SE)? Q) How does the system account for premature infants? Q) How do we screen a child that has a previously identified delay? Measure 13: Behavioral Concerns & Home Visits Definition: Percent of home visits where primary caregivers were asked if they have any concerns regarding their child’s development, behavior, or learning. Caregiver Measure. M13 Behavioral Concerns & Home Visits FAQ's When is this collected? How is this calculated for reporting purposes? Q) Is the behavioral concerns question collected regardless of the age of the child? Q) How are alternative visits counted such as Telehealth / Virtual Home Visiting? Q) Should we be entering Measure 13 for all Telehealth or virtual visits? Q) Should it be a pre-natal visit if the Caregiver has an enrolled child and the Caregiver is also pregnant? Q) If the Caregiver has multiple children how do we count visits? Measure 14: Intimate Partner Violence (IPV) Screening Definition: Percent of primary caregivers enrolled in home visiting who are screened for intimate partner violence (IPV) within 6 months of enrollment using a validated tool. Caregiver Measure. Validated Screening Tools Please note as of 10/1/21 the following tools are no longer consider validated tools for the purpose of this data collection. Abuse Assessment Screen (AAS) Abusive Behavior Inventory (ABI) Composite Abuse Scale (Revised)─Short Form (CASR-SF) – Added 10/1/2021 Conflict Tactics Scales – Revised (CTS) – Added 10/1/2021 Domestic Violence Screening for Pediatric Settings – Added 10/1/2021 Harassment in Abusive Relationships: A Self-Report Scale (HARASS) Humiliation, Afraid, Rape, Kick, Child (HARK-C) Humiliation, Afraid, Rape, Kick, Child (HARK-C) Hurt, Insulted, Threatened with Harm and Screamed (HITS) Ongoing Abuse Screening (OAS) Partner Violence Screen (PVS) Profile of Psychological Abuse of Women (PPA) Relationship Assessment Tool (formerly the Women’s Experience with Battering [WEB]) – Name Changed 10/1/2021 The Relationship Chart Universal Violence Prevention Screening Protocol – Adapted Women Abuse Screening Tool (WAST) M14 IPV Screening FAQ's When is this collected? How is this calculated for reporting purposes? Q) If the Caregiver is not in a relationship do I screen? Q) What screening tool should Nurse-Family Partnership (NFP) select in the system? Measure 15: Primary Caregiver Education Definition: Percent of primary caregivers who enrolled in home visiting without a high school degree or equivalent who subsequently enrolled in, maintained continuous enrollment in, or completed high school or equivalent during their participation in home visiting. Caregiver Measure. M15 Primary Caregiver Education When is this collected? How is this calculated for reporting purposes? Q) When Update is Selected Measure 15 shows up again? Measure 16: Insurance Coverage Definition: Percent of primary caregivers enrolled in home visiting who had continuous health insurance coverage for at least 6 consecutive months. Caregiver Measure. M16 Insurance Coverage FAQ's When is this collected? How is this calculated for reporting purposes? Q) How is continuous coverage defined? Measure 17: Completed Depression Referral Definition: Percent of primary caregivers referred to services for a positive screen for depression who receive one or more service contacts. M17 Completed Depression Referrals FAQ's When is this collected? How is this calculated for reporting purposes? Q) Can we exclude those who have already been referred to services? Q) What are some examples of recommended services for depression? Q) If a participant calls the hotline (currently available for MIECHV funded participants) would that be considered as receiving a service for PM17? Measure 18: Completed Developmental Referral Definition: Percent of children enrolled in home visiting with positive screens for developmental delays (measured using a validated tool) who receive services in a timely manner. M18 Completed Developmental Referrals FAQ's When is this collected? How is this calculated for reporting purposes? Measure 19: IPV Referrals Definition: Percent of primary caregivers enrolled in home visiting with positive screens for IPV (measured using a validated tool) who receive referral information for IPV. Caregiver Measure. M19 IPV Referrals When is this collected? How is this calculated for reporting purposes? Measure 20: Substance Use Screenings (Optional as of 10/1/21) Definition: Number of primary caregivers enrolled in home visiting who were screened for both unhealthy alcohol use and drug use using validated tool(s) within 6 months of enrollment. Caregiver Measure. Validated Tools The Alcohol Use Disorders Identification Test-Concise (AUDIT-C) The Alcohol Use Disorders Identification Test Self-Report (AUDIT Self-Report Version) The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) The Alcohol, Smoking, and Substance Involvement Screening Test- Frequency & Concern Items (ASSIST-FC) Cut Down, Annoyed, Guilty, Eye opener -Adapted to Include Drugs (CAGE-AID) The Drug Abuse Screening Test (DAST-10) National Institute on Drug Abuse (NIDA) Quick Screen Parents, Partners, Past and Pregnancy (The 4Ps) Plus Tolerance Annoyance Cut Down Eye Opener (T-ACE) Tolerance, Worried, Eye-opener, Amnesia, Cut Down (TWEAK) Used, Neglected, Cut Down, Objected Preoccupied, Emotional Discomfort (UNCOPE)* M20 Substance Use Screenings FAQ's When is this collected? How is this calculated for reporting purposes? Q) Are all OCDEL funded EBHV expected to complete this measure? Q) How is unhealthy alcohol use and drug use defined? Q) Do I need to complete more than one tool? Q) Can you turn off the substance use screening performance measures for the whole agency or will staff have to answer them each time that we are not participating in the substance use screenings? Measure 21: Substance Use Referrals (Optional as of 10/1/21) Definition: Number of primary caregivers enrolled in home visiting who received recommended services for substance use (and met the conditions specified in the denominator). M21 Substance Use Referrals FAQ's When is this collected? How is this calculated for reporting purposes? Q) What are recommended services defined as? Funded Slots and Goals Change Request Form Step 1: Select Funded Slots from the Enrollment Report List. Step 2: Select the link to request an update. Can also view prior updates and history by selecting update history. Step 3: All fields can be updated as necessary, except for fiscal year. Step 4: Complete the following text box and question responses with the appropriate information. Step 5: Once the request is submitted it goes to the Family Support Program Consultants or Children’s Trust Fund TA Staff for initial approval. Step 6: Following their initial approval it is then approved by the Family Support Program Data Analyst for data collection and report tracking. Step 6: The Agency Admin will receive an email with the approval or rejection at either Step 5 or 6. Please be sure to add: phv@csc.csiu.org to your contact lists to ensure all emails from the data system are received. Enrollment Report Overview Video Requirements to Generate the Enrollment Report All demographic data for Caregivers and Children enrolled in services shall be entered into the Family Support Data System no later than the 10th of the month following their enrollment. As an example: if a family enrolls in services in October they would be entered into the data system by no later than November 10th. Generating the Enrollment Report Step 1: Under the Report List on the Agency Dashboard there will be an option to Generate Enrollment Report Month. Click on the link. Step 2: Please select the Month and Year of the Enrollment Report you would like to generate. Please note that enrollment reports will be generated for all Program Types Funded Slots are assigned to. Step 3: Once the report is generated the system will bring you back to the Agency Dashboard Page. Step 4: View the Report under the appropriate enrollment link(s) and edit as required. Step 5: Reports are not considered submitted until they have been edited. Step 6: Select Submit to submit and lock the report. Step 7: If the report needs to be unlocked you may email your Family Support Consultant or the RA Account to unlock the report after submission. Deleting an Enrollment Report If a month is generated erroneously it can be deleted prior to submission. The enrollment report must be deleted prior to the submission (edits). Q) Who can delete the report? Exporting the Enrollment Report Step 1: Select Export Enrollment Report at the bottom of the report list Step 2: Choose Date Range Step 3: The Document will Export to Excel as a Download. Program Types (Funding) tabs will be at the bottom. Enrollment Report Definitions Enrollment – Families are considered “enrolled” when they have formally agreed to participate in the program when they complete the intake process and are participating in the program as required by the Agency. All household members receiving home visiting services count as one family. The number of family members enrolled could vary from family to family but will involve at least one (e.g., pregnant caregiver) or two (parents plus child) clients, both of these examples would be considered one family each. Report Date – Month and Date of the Report Model – EBHV or Family Support Program Model County – County in which the services are being provided Funded Slots – Maximum number of families (slots) that can be served at one time agreed upon by your agency and OCDEL through your grant agreement or updated work-statement. The number of slots should remain the same throughout the grant unless a program revision is submitted and approved. Goal Number of Families to be Served – Total number of families that will be served over the course of the fiscal year. Goal Number of Parents/Caregivers to be Served – Total number of parents/caregivers that will be served over the course of the fiscal year. Goal Number of Children to be Served – Total number of children that will be served over the course of the fiscal year. Number of Continuing Families as of the End of the Month – Number of families continuing from before the reporting month that were enrolled as of the end of the reporting month. Does not include families that exited during the reporting month. Total Number of New Families as of the End of the Month – This should capture only the new families that were enrolled as of the end of the month and are considered new if they enrolled within the reporting month. Cumulative Number of Families Served to Date as of the End of the Month (Unduplicated) – Total number of families that have ever received services, this number does not decrease. Number of cumulative families equals the prior months cumulative number of families plus the new families enrolled in the month that is being reported on. Number of Families Exited as of the End of the Month – Completed Program – Those who have fully completed the program model as specificed by each individual model. Number of Families Exited as of the End of the Month – All other Reasons – Any families that were exited that did not complete the program as specified by each individual model. Number of Families On Hold as of the End of the Month – Families placed on hold in the system. Number of Children Enrolled as of the End of the Month – The number of children being served. Not including those who are under the age of adulthood who are parents. Does not include prenatal. Number of Prenatal Children – This is the number of children in utero. This is calculated by using the Number of Prenatal Caregivers, if the Caregiver is expecting multiple children (twins, etc) they would be counted as two children in this section. Cumulative Number of Children Served to Date as of the End of the Month (Unduplicated) – Total number of children that have ever received services, this number does not decrease. Barriers to Establish Full Enrollment / Extenuating Circumstances – Use this section to discuss any concerns, updates, circumstances, etc. regarding low enrollment within the program. Date when Full Enrollment is Expected – Date when the program is expected to be fully enrolled. Comments/ Edit Comments (Barries to Meeting Goals/Comments) – Use this space to discuss any additional comments or describe any edits that were made to the enrollment report. Staff Reporting Overview Video Entering the Staffing Report Step 1: Click the link for the Staffing Report in the Report List Step 2: Scroll down to enter the Staffing Report Step 3: Select the Month and Year of the Report based on the due dates Step 4: Complete the remaining information Step 5: Submit the Report Copying the Prior Reports Copying: If no changes from last report, click the copy button at the left hand side of each of the rows, this will autofill all data except the date of report and comments. Add date of report and comments (if desired or warranted) and click submit at the bottom of the page. Deleting the Staffing Report The Agency Administrator, Data User, and Supervisor Roles can delete the report if there is any accidental entry. They can also edit reports if a change is needed. Step 1. Select Delete Step 2. Confirm that the report should be delete by selecting yes. Staffing Report Definitions Date of Staffing Report – Date Report is being Submitted Note: Home Visitors in the definitions below also include Family Support Staff for non EBHV programs Total Overall Number of Home Visitors (Not Vacant) – Physical Count of Home Visitors employed under the program type selected. Total Overall Home Visitors should only include whole numbers. It is okay if a single person is counted twice due to being funded by more than one program type. Total Overall Number of Vacant Home Visiting Staff – Physical Count of open positions for Home Visitors that would employed under the program type selected if hired. Total Vacant Staff should only include whole numbers. It is okay if a single vacant posiiton is counted twice due to being funded by more than one program type. New Full-Time Equivalent (FTE) Continuing Full-Time Equivalent (FTE) Vacant Full-Time Equivalent (FTE) FTE Calculation Quarterly Narrative Overview Video Updated video coming soon. Quarterly Narrative Template Note: To be considered submitted timely the official submission must be received through the Family Support Data system. This template is only being provided to help with collection of the data throughout the quarter. Entering the Quarterly Narrative Do not exceed 60 Minutes or the reports will not save. Step 1: Select Quarterly Narrative from the Report List Step 2: Generate the Report by selecting the Quarter End Date and Calendar Year Step 3: Enter all relevant information regarding your current EBHV, Family Support Programs, and Funding Step 4: To respond to a specific section you can hover over the header to determine what is needed in the response. Step 5: Once all areas have been completed you may submit the report. Please note if you Save the Report that does not finalize the submission. Step 6: If you are receiving MIECHV or CBCAP American Rescue Plan funding, select Yes on the supplemental questions to complete those sections of the report. Step 7: If you have saved the report and want to continue to edit you will have to select edit on the report list. Step 8: Once finalized click Submit. The report will then be reviewed by your designated Family Support Consultant or TA from the Center for Schools and Communities, they may add comments. You can view the comments by scrolling to the right on the report list. Deleting the Quarterly Narrative Step 1: If you add a Quarterly Narrative with the wrong date by mistake you can delete it from your list. As long as you have not submitted it. In the example below you can see the bottom report in the list does not have delete as it has been submitted. Step 2: After selecting delete confirm that you wish to delete the report by selecting yes. Quarterly Narrative Definitions To respond to a specific section you can hover over the header to determine what is needed in the response. Monthly Reports Entered for each Family, Caregiver, and Child, Updated as needed*, and at exit from program. Entered for each primary parent/caregiver and child(ren) at the appropriate timelines based upon enrollment in evidence-based home visiting programs. Programs should attempt to complete all Performance Measures and not skip a screening because it does not fall on the exact date in the data system. Every Other Month Reports Quarterly Reports Twice a Year Reports Demonstrates progress toward outcomes and indicators. Submitted through the CTF Uploader. Yearly Reports As Needed or Required Reports Agency Demographic Export The report is named “Demographics Export” on the Report List on the Agency Dashboard, and is available to Agency Administrator and Agency Data user types. These two types have access to all family data for an agency. Contact the RA Account if you believe you need a different user type. The reporting period dates determine which families are included in the demographics export. The export will include Children and Caregivers who were actively enrolled at any point during your chosen reporting period. This is the county of residence entered as part of the Caregiver’s address. For Children, the Caregiver’s county of residence is used. Currently, program type and funding are required entries, meaning that each export can only include data for families enrolled in one program and one funding type. After a few seconds, an Excel file titled “AgencyDemographicsExport” will be downloaded containing your Demographic data. Count of Participants – Included: All Primary Caregivers and Children matching the chosen export criteria Primary Caregivers by Age – Included: All Primary Caregivers matching the chosen export criteria Children by Age – Included: All Children matching the chosen export criteria Participants by Ethnicity – Included: All Primary Caregivers and Children matching the chosen export criteria Participants by Race – Included: All Primary Caregivers and Children matching the chosen export criteria Marital Status – Included: All Primary Caregivers matching the chosen export criteria Education Attainment – Included: All Primary Caregivers matching the chosen export criteria Measure Fifteen (EBHV Programs only) – Included: Primary Caregivers that did not have a high school diploma or equivalent at enrollment. Measure fifteen is collected as part of the Caregiver demographics though it is an EBHV Performance Measure. Education Status – Included: All Primary Caregivers matching the chosen export criteria Employment Status – Included: All Primary Caregivers matching the chosen export criteria Housing Status – Included: All Primary Caregivers matching the chosen export criteria Primary Language Spoken at Home – Included: All Children matching the chosen export criteria Household Income – Included: All Families matching the chosen export criteria Priority Populations Tables – Included: All Families matching the chosen export criteria
Status or Exit Reason – Included: All Families matching the chosen export criteria This table displays the current status of each family, as of the date you download the export. If the family is not active or on hold, the Exit Reason is listed. Health Insurance – Included: All Primary Caregivers matching the chosen export criteria Source of Medical Care – Included: All Primary Caregivers matching the chosen export criteria Source of Dental Care – Included: Children above 1 year of age matching the chosen export criteria Low Birth Weight – Included: Children of primary caregivers who enrolled prenatally Prenatal Substance Exposure – Included: Children of primary caregivers who enrolled prenatally Safe Care Plan – Included: Children who were born affected by prenatal substance exposure
Update Password/Forgot Password / Password Reset
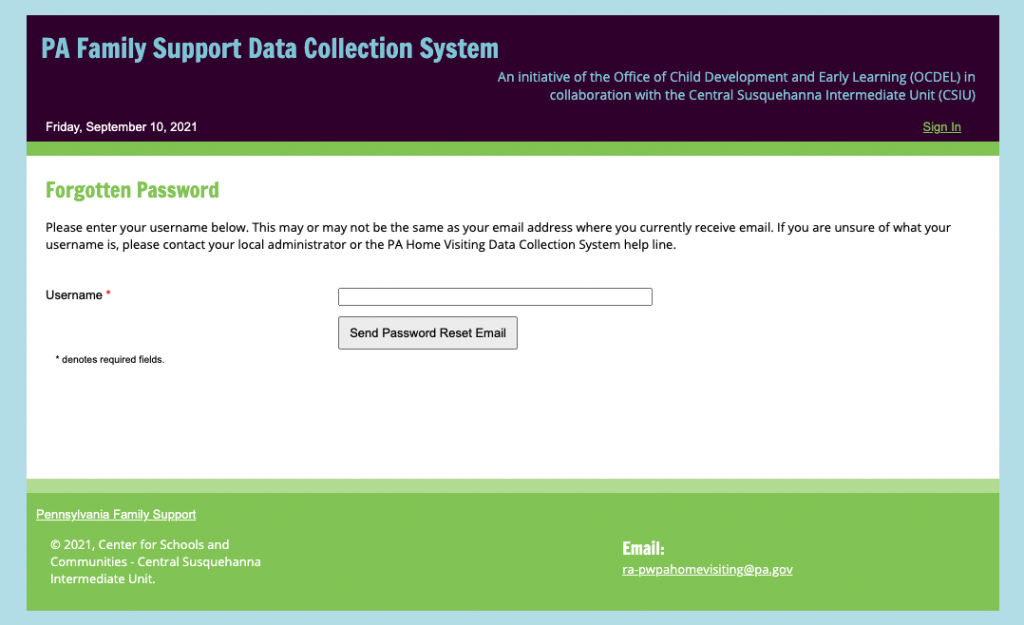
The subject of the email will be: Your Request to Reset Your PA Home Visiting Data Collection System Password.
The password reset email will be from: PHV@CSC.CSIU.ORG (please do not email this account as it is not monitored).
Definition: These are the staff that are providing direct EBHV or Family Support Services to Families that do not currently hold a supervisory role.
Roles: The Home Visitor in the Pennsylvania Family Support Data System allows the person in this role to add and update families currently served by them.
Additional Permissions: The Home Visitor Role has the ability to remove accidental family entries if no Caregiver demographics have been entered. Please see removing Accidental Entries below for additional guidance.
Definition: These are the staff that currently hole a supervisory role, they may or may not provide EBHV and Family Support services directly to families. This role is for Supervisors that manage a portion of the Home Visitors or Family Support Providers within an Agency.
Roles: The Home Visitor Supervisor in the Pennsylvania Family Support Data System allows the person in this role to add and update families currently served by them. They are also able to view the families of the Home Visitors they supervise. The Supervisor must have a Data User or Agency Administrator link the Home Visitors they supervise directly to them. Please see Linking Users to Families below for additional guidance.
Additional Permissions: The Home Visitor Supervisor role is view and submit Programatic reports. Please see the Programatic Report section below for additional guidance.
Definition: The staff person within an agency responsible for the fiscal reporting. This person only works with the fiscal aspects of the EBHV or Family Support program.
Roles: The Agency Fiscal role only has access to the budget, fiscal reporting templates. They complete the budget, budget narrative, and all fiscal reports for the program fiscal year.
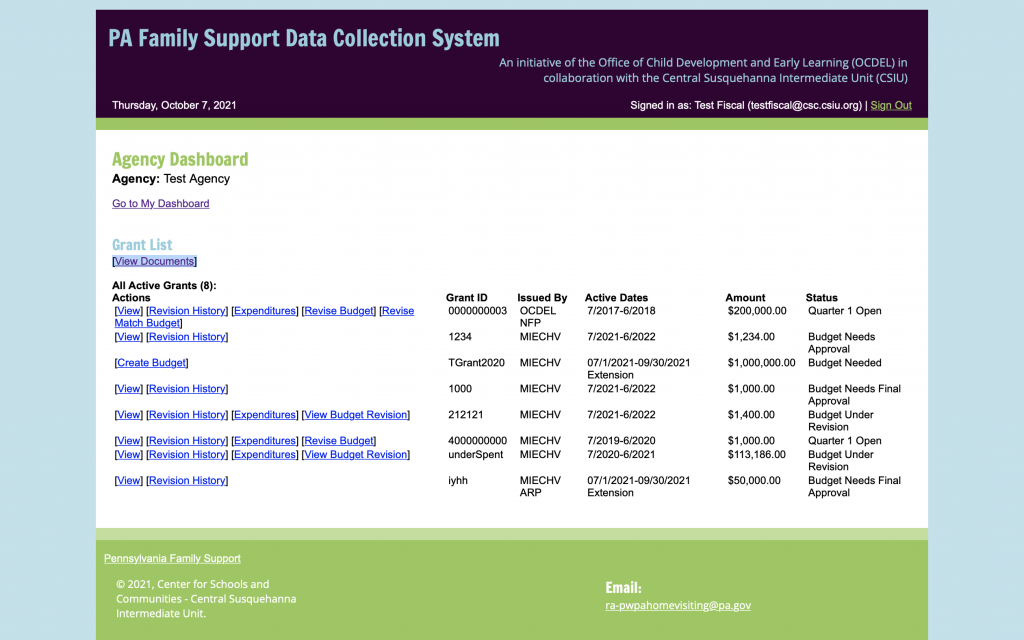
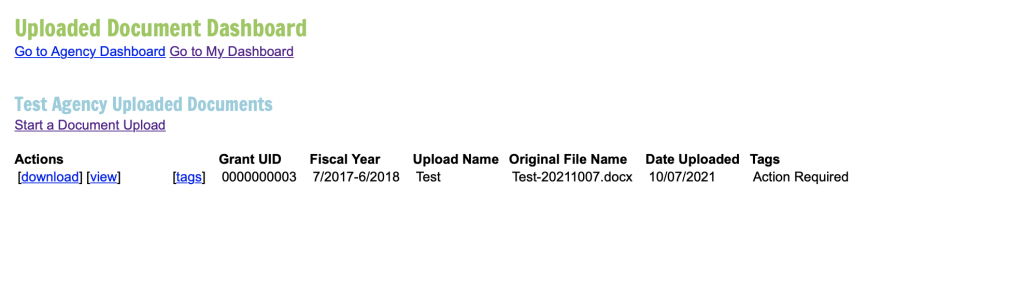
Additional Permissions: The Agency Fiscal role has the ability to upload and download documents added to the data system under the Grant List at the View Documents tab. Please see the Document Uploader section, under the header Overview of the Dashboards, below for additional guidance.
Definition: The staff person within an agency responsible for the data reporting and entry.
Roles: The Agency Data User has access to all families and programatic reports. The Agency Data User Role does not have access to fiscal information.
Additional Permissions: The Agency Data User has access to all families, has access to link Families to Supervisors and Home Visitors and has the ability to delete existing families from data system. Please see removing Accidental Entries below for additional guidance.
Definition: The Agency Administrator is the leader responsible for the implementation of the program.
Roles: The Agency Administrator has access to all families and programatic reports. The Agency Data User Role has access to all fiscal information.
Additional Permissions: The Agency Data Administration has access to all families, has access to link Families to Supervisors and Home Visitors and has the ability to delete existing families from data system. Please see removing Accidental Entries below for additional guidance. The Administrator role also has the ability to deactivate staff.
Overview and Navigation of the Dashboards
The Agency Administrator role has the ability to deactivate users. If selected it will prompt them to confirm. If a user is deactivated and then later returns to the Data System an email to the RA Account will be required to reinstate their account. 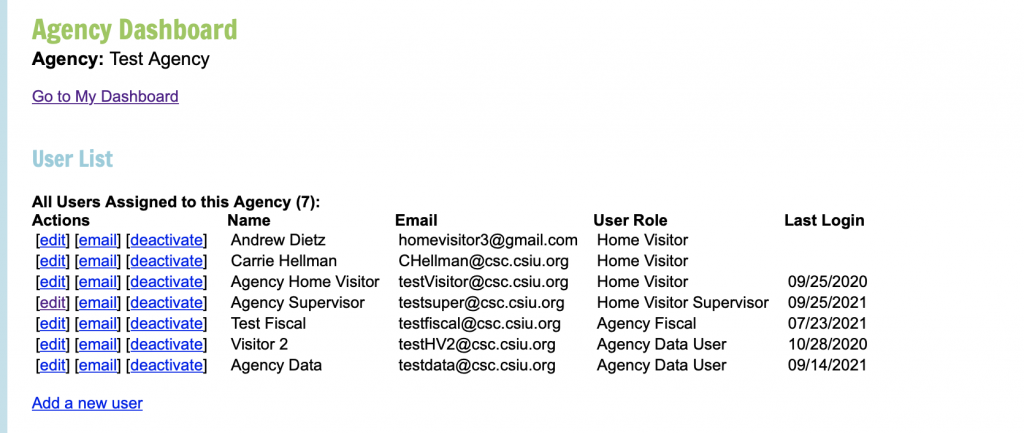
The Agency Data User role has the ability to deactivate users. If selected it will prompt them to confirm. If a user is deactivated and then later returns to the Data System an email to the RA Account will be required to reinstate their account. 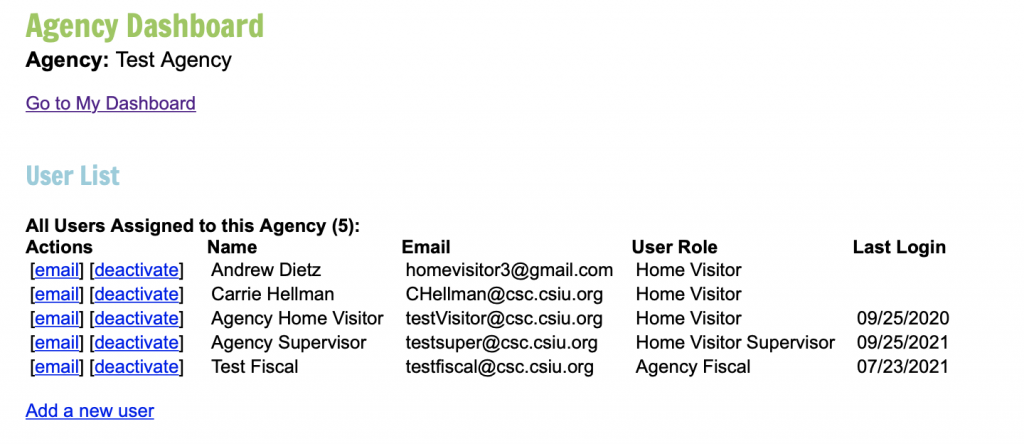



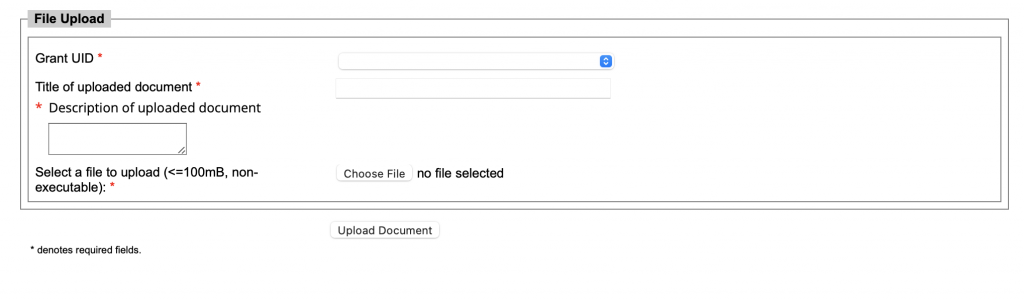
1. Scroll down to Grant List
2. Click on the link to View Documents
3. Click on the Start a Document Upload
4. Select Grant ID
5. Provide a clear Title for the Document
6. Provide a clear description for the Document
7. Select the file.
8. Click the link to upload the document.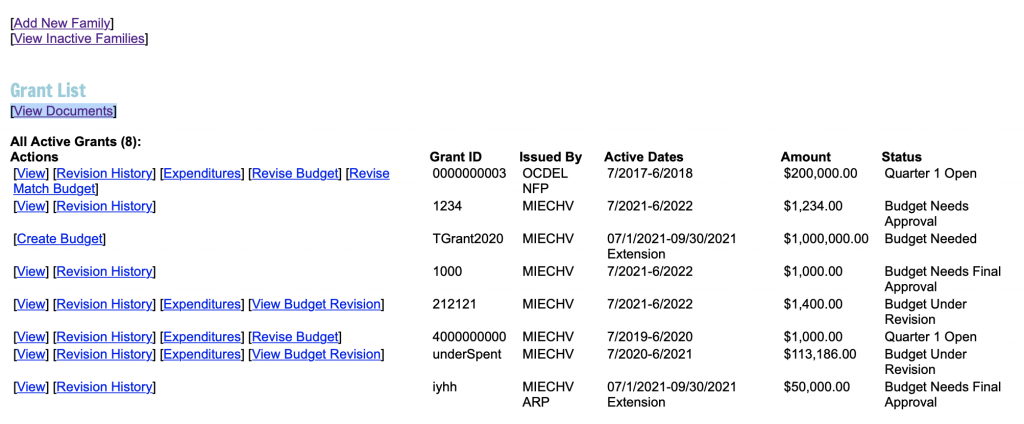
Data Entry Guidance
If requesting a transfer Please email the RA Account with the following:
– Original Agency
– Name of the Primary Caregiver
– New Agency, and
– Assigned home visitor if applicable.
As an example if Family A is currently enrolled in NFP in Montgomery County and plans to continue receiving NFP services in Columbia County after moving through the NFP agency in that area that families record can be transferred between the two agencies.
Please note: That most families when moved are found on the inactive list at the new agency and will need to be un-exited. Please use the date of the transfer to the new provider as the un-exit date, this will clear any overdue or missing measures. 
Enrollment & Demographic Definitions and FAQ’s
At Enrollment
Update between June 1st and June 30th each year.
Update between Sept 1st and Sept 30th each year.
The 10th of the next month if notified of a change
Entries Marked with * are required
Number of People in Household Clarifications
– The child is only included in this number once they are born.
– Additional children living in the home should be counted (even if not enrolled in the EBHV or Family Support Program). These additional Child(ren) should not be entered into the data system unless they are considered enrolled in the EBHV and/or Family Support Program(s).
Q) What is the definition of Financial Support
A) Financial Support is Strictly Monetary, it does not include shelter, food, etc…
Income Calculations Guidelines
– The economic response / stimulus payments are not part of gross income and would not be included in the income calculation.
– Unemployment benefits are considered part of gross income per the IRS, so these would be included when calculating household income.
NFP Choices | Family Support Data System Choices
Client is dependent on p/g | Report as Less than or equal to $6,000
Less than or equal to $6,000 | Less than or equal to $6,000
$9,001-$12,000 | $6,001-$12,000
$12,001-$16,000 | $12,001-$20,000
$16,001-$20,000 | $12,001-$20,000
$20,001-$30,000 | $20,001-$30,000
Over $30,000 | $30,001 to $40,000
If Client discloses over $40,000 | Over $40,000
For NFP if the NFP Client is dependent upon their Caregivers income you should still choose $0 to $6,000 in the system unless the NFP Client discloses their Caregivers income then you should choose the most accurate response.
Tobacco use is defined as: combustibles (cigarettes, cigars, pipes, hookahs, bidis), non-combustibles (chew, dip, snuff, snus, and dissolvables), and electronic nicotine delivery systems (ENDS).
Clarifications
– Use of Tobacco Products it not limited to only physical use inside the home.
– When answering this question, consider anyone who is living in the home. Please note that these answers will not be compared to the answer for “Number of People in Household”
Options include
Court System (Judge) – A Judge recommended that the Family Receive Family Support Services, all OCDEL funded Family Support Programs are voluntary and should not be ordered by a Judge but in some circumstances may be recommended.
Children and Youth – Referral from Children and Youth
Department of Corrections (DOC) – Referral from the Department of Corrections
Doctor’s Office – Referral from a Doctor’s Office
Early Intervention (EI) – Referral from an Early Intervention Provider
Early Learning Resource Center (ELRC) – Referral from an ELRC
Hospital – Referral from a Hospital
Managed Care Organization – Referral from one of the Managed Care Organizations. All MCO’s are listed within this option.
Other Home Visiting or Family Support Program – Referral from another Home Visiting or Family Support Program.
Self-Referral – Family Called, Emailed, Texted, Etc. and requested the services themselves
Women, Infant, and Children (WIC) – Family was referred to the Family Support program by WIC
Word of Mouth – Family was referred to program by another family. Two options under this section are:
– – Current Participant in Services
– – Prior Participant in Services
Other – Use this section to fill in any additional referral sources that are not listed above, we will review this and add additional options are appropriate.
At Enrollment
Entries Marked with * are required
Caregiver must be enrolled in an EBHV program or a Family Support Program or Both
Caregiver can be enrolled in one EBHV program and up to four Family Support Programs
Clarifications
Caregiver must be enrolled in an EBHV program or a Family Support Program or Both
Caregiver can be enrolled in one EBHV program and up to four Family Support Programs
Transfers
If a Family was transferred from a different Agency their original enrollment date in the EBHV or Family Support Program should be used as the enrollment date in the new agency.
If your agency is receiving a transfer family or transferring a family to another agency, please contact the RA Email Account.
Multips Pilot (NFP Only)
The system will ask if the Caregiver is also enrolled in the Multips Pilot.
Multips Pilot (NFP Only) Enrollment Date
If enrolled in the Multips Pilot this may be the same date as the enrollment date for NFP.
or
If enrolled with a second child with a child already receiving NFP services this should be the date the family enrolled in the Multips pilot.
Multips: Case ID for Second Child
Use the second NFP ID for the Child Case ID once they are born and entered into the system.
Multips: First Child Graduation
If the initial Child graduates they can be exited with the reason of Completed Program while the Caregiver and Multips Child remain enrolled.
At Enrollment or Within 15 Days of Enrollment
Update between June 1st and June 30th each year.
Update between Sept 1st and Sept 30th each year.
The 10th of the next month if notified of a change
Entries Marked with * are required
Clarifications
Zip Codes: Please note that when entering Zip Codes. That they can only be 5 digits, entering more than 5 digits will cause the demographic information to not save.
Q) What address do I use if the Caregiver is homeless and has not identified an address?
A) You may use the address of your Agency or Local County Office if applicable
Q) If the Caregiver is in prison / jail what address do I use?
A) You may use the address of the prison / jail for the Caregiver
Female caregivers – are those household members who identify as female and who are enrolled in the program during the reporting period, are considered a caregiver of the index child (e.g., biological parent, adoptive parent, foster parent, grandparent who identifies as female).
Male caregivers – include those household members who identify as male and who are enrolled in the program during the reporting period, are considered a caregiver of the index child, and (e.g. biological parent, step-parent, and partners who identify as male) who also meet the definition of an enrollee.
Gender Non-Binary (Caregivers) – includes those enrolled participants who also meet the definition of an enrollee and who do not identify as either male or female, which may include participants who identify as gender non-binary and/or genderqueer.
Resources: Here are some other resources that may be helpful in having home visitors become more knowledgeable on the topic:
– A Guide to Gender Identity Terms
– Overview and a guide to being an ally
– Gender Unicorn (visual guide)
– What are pronouns and why do they matter?
– 3 myths about transgender youth
– Video: The Science of Being Transgender
– Free Webinars
– Center for the Study of Social Policy “Our Identities, Ourselves” – http://www.pa-home-visiting.org/wp-content/uploads/2021/11/Our-Identities-Ourselves-Data-Collection-Guide.pdf
– Center for the Study of Social Policy “Our Identities, Ourselves” – Literature Review – http://www.pa-home-visiting.org/wp-content/uploads/2021/11/Our-Identities-Ourselves-Literature-Review.pdf
Clarifications
Nurse-Family Partnership – Because this Model does not serve the second child (unless participating in Multips) the Caregivers Status Should Not be updated to Pregnant if Pregnant with a second child as this will cause PM’s to show that are not applicable.
However if the Caregiver is participating in the Multips Pilot with the Second Child then their pregnant status should be updated.
(3) Child with a disability.
(A) In general.–The term `child with a disability’ means a child
(i) with mental retardation, hearing impairments (including deafness), speech or language impairments, visual impairments (including blindness), serious emotional disturbance (referred to in this title as `emotional disturbance’), orthopedic impairments, autism, traumatic brain injury, other health impairments, or specific learning disabilities; and
(ii) who, by reason thereof, needs special education and related services.
(B) Child aged 3 through 9. The term child with a disability’ for a child aged 3 through 9 (or any subset of that age range, including ages 3 through 5), may, at the discretion of the State and the local educational agency, include a child
(i) experiencing developmental delays, as defined by the State and as measured by appropriate diagnostic instruments and procedures, in 1 or more of the following areas: physical development; cognitive development; communication development; social or emotional development; or adaptive development; and
(ii) who, by reason thereof, needs special education and related services.
And from Part C, Section 632(5) which is:
(5) Infant or toddler with a disability. The term `infant or toddler with a disability'(A) means an individual under 3 years of age who needs early intervention services because the individual
(i) is experiencing developmental delays, as measured by appropriate diagnostic instruments and procedures in 1 or more of the areas of cognitive development, physical development, communication development, social or emotional development, and adaptive development; or
(ii) has a diagnosed physical or mental condition that has a high probability of resulting in developmental delay.
More information here: https://www.dhs.pa.gov/KeepKidsSafe/About/Pages/Plans-of-Safe-Care.aspx
Clarifications
Current official legal status, meaning if Currently Divorced but living with a new partner this would be entered as Divorced.
Currently enrolled in Middle School includes individuals who are enrolled in Middle School.
Currently enrolled in High School includes individuals who are enrolled in High School.
Currently enrolled in a GED Program includes individuals who are enrolled in a GED Program.
Less than high school diploma includes individuals who have not completed their high school education and are not currently enrolled in school or a GED program.
The Some college/training category includes those who are currently enrolled and those who attended in the past.
The Technical training or certification category includes those who received technical training or certification in the past.
The Associate’s Degree category includes those who obtained an Associate’s Degree.
The Bachelor’s Degree or Higher category includes those who obtained a Bachelor’s Degree or a higher degree.
The Other category includes those individuals who did not fall into the specified categories.
Clarification
Caregivers should be entered / updated to reflect their current status as it relates to employment, once the home visitor or family support staff is notified of the change.
Q) Due to the current situation (COVID-19) we were wondering how unemployment should be recorded right now? We have several Caregivers across programs who are laid off but will be going back when businesses reopen. Should that be considered unemployed?
A) Caregiver who is currently laid off and not working would be considered “not employed”.
Homeless: Individuals who lack a fixed, regular, and adequate nighttime residence (with the meaning of section 103(a)(1) of the McKinney-Vento Homeless Assistance Act).
Homeless and sharing housing: Individuals who are sharing the housing of other persons due to loss of housing, economic hardship, or a similar reason.
Homeless and living in an emergency or transitional shelter: Individuals who are living in emergency or transitional shelters; are abandoned in hospitals; or are awaiting foster care placement.
Some other Arrangement: Individuals who are living in motels, hotels, trailer parks, or camping grounds due to the lack of alternative adequate accommodations; individuals who having a primary nighttime residence that is a public or private place not designed for ordinarily used as a regular sleeping accommodation for human beings (with the meaning of section 103(a)(2)(C)); individuals who are living in cars, parks, public spaces, abandoned buildings, substandard housing, bus or train stations or similar settings.
Q) What do I choose if a client has a primary and secondary insurance?
A) Select the Primary Insurance
Measure 15 Question: Have you (caregiver) enrolled in, maintained continuous enrollment in, or completed a high school degree or equivalent?
– Select Yes if Caregiver maintained enrollment in school or GED program or newly enrolled in school or a GED program.
– Select No if Caregiver is not enrolled and has less than a High School Diploma or Equivalent (GED)
At Enrollment or first visit after birth if caregiver enrolled prenatally
Update between June 1st and June 30th each year.
Update between Sept 1st and Sept 30th each year.
The 10th of the next month if notified of a change
Entries Marked with * are required
Clarifications
NFP Multips – If a Client is dually enrolled in base NFP and Multips NFP when the second Child is born use the Multip ID as the second Childs ID.
Note: For Child Gender you may use the gender assigned at birth for the Child unless the caregiver requests to use the non-binary option, then select that as the response.
Female child – are those children who identify as female and who are enrolled in the program during the reporting period.
Male child – are those children who identify as as male and who are enrolled in the program during the reporting period.
Gender Non-Binary (Child) – includes those enrolled children who also meet the definition of an enrollee and who do not identify as either male or female, which may include participants who identify as gender non-binary and/or genderqueer.
Resources: Here are some other resources that may be helpful in having home visitors become more knowledgeable on the topic:
– A Guide to Gender Identity Terms
– Overview and a guide to being an ally
– Gender Unicorn (visual guide)
– What are pronouns and why do they matter?
– 3 myths about transgender youth
– Video: The Science of Being Transgender
– Free Webinars
– Center for the Study of Social Policy “Our Identities, Ourselves” – http://www.pa-home-visiting.org/wp-content/uploads/2021/11/Our-Identities-Ourselves-Data-Collection-Guide.pdf
– Center for the Study of Social Policy “Our Identities, Ourselves” – Literature Review – http://www.pa-home-visiting.org/wp-content/uploads/2021/11/Our-Identities-Ourselves-Literature-Review.pdf
– Parental Acceptance of Gender Expression
Home visitors are uniquely positioned to support parental acceptance of their children’s gender expression, yet not always prepared to do so. Parental acceptance is associated with improved self-esteem and lower rates of depression and suicidality among children, and better family relationships, overall. Parental Acceptance of Gender Expression in Young Children includes information on gender and gender development, strategies home visitors can use to support gender acceptance among parents, and opportunities for awardees to support LIAs in these efforts. Also included are resources for families, including a handout that home visitors can share with parents and caregivers.
Clarifications
Enter a whole number for lbs and a whole number for oz. Do not enter any decimals or letters within these text boxes.
Clarifications
Enter a whole number for Weeks and a whole number for days. Do not enter any decimals or letters within these text boxes.
(3) Child with a disability.
(A) In general.–The term `child with a disability’ means a child
(i) with mental retardation, hearing impairments (including deafness), speech or language impairments, visual impairments (including blindness), serious emotional disturbance (referred to in this title as `emotional disturbance’), orthopedic impairments, autism, traumatic brain injury, other health impairments, or specific learning disabilities; and
(ii) who, by reason thereof, needs special education and related services.
(B) Child aged 3 through 9. The term child with a disability’ for a child aged 3 through 9 (or any subset of that age range, including ages 3 through 5), may, at the discretion of the State and the local educational agency, include a child
(i) experiencing developmental delays, as defined by the State and as measured by appropriate diagnostic instruments and procedures, in 1 or more of the following areas: physical development; cognitive development; communication development; social or emotional development; or adaptive development; and
(ii) who, by reason thereof, needs special education and related services. And from Part C, Section 632(5) which is: (5) Infant or toddler with a disability.–The term `infant or toddler with a disability’
(A) means an individual under 3 years of age who needs early intervention services because the individual
(i) is experiencing developmental delays, as measured by appropriate diagnostic instruments and procedures in 1 or more of the areas of cognitive development, physical development, communication development, social or emotional development, and adaptive development; or
(ii) has a diagnosed physical or mental condition that has a high probability of resulting in developmental delay.
Q) What do I choose if a child has a primary and secondary insurance?
A) Select the Primary Insurance
Q) What is the answer for usual source of dental care for a newborn?
A) The answer is No. This question only applies after the Child turns 1 year of age. When updating the child after the child has turned 1 if a usual source of dental care has been identified the answer should be updated to Yes.
Performance Measures Definitions and FAQ’s
Collected via the demographics.
Preterm birth is defined as a birth before the 37 completed weeks of gestation (defined as up to 36 weeks and 6 days). The “37 completed weeks” means 36 weeks and 7 days.
NUMERATOR: Number of live births (index child or subsequent children among mothers who enrolled in home visiting prenatally before 37 weeks) born before 37 completed weeks of gestation and after enrollment.
DENOMINATOR: Number of live births after enrollment who were born to mothers enrolled in home visiting prenatally before 37 weeks.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: N/A
To be included in the reporting period, participants need to have enrolled prior to 37 completed weeks of gestation and delivered the baby during the reporting period. If the participant enrolls prior to 37 weeks in the current reporting period but delivers in the subsequent reporting period, the participant will be included in the subsequent reporting submission. If she enrolls prior to 37 weeks in the previous reporting period but delivers in the current reporting period, she will be included in the current report submission.
Only if Caregiver Enrolled Prenatally. 3 Months Post Enrollment of Child using their date of birth (DOB) and 6 Months Post Enrollment of Child using their DOB. Children cannot be enrolled in the EBHV model prior to their DOB).
NUMERATOR: Number of infants aged 6-12 months (index child among mothers who enrolled in home visiting prenatally) who were breastfed any amount at 6 months of age.
DENOMINATOR: Number of infants aged 6-12 months (index child among mothers who enrolled in home visiting prenatally) enrolled in home visiting for at least 6 months.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: Caregivers with a Medical issue as defined below are excluded from the calculation.
Infected with human immunodeficiency virus (HIV), Taking antiretroviral medications, have untreated, active tuberculosis, infected with human T-cell lymphotropic virus type I or type II, Using or is dependent upon an illicit drug, taking prescribed cancer chemotherapy agents, such as antimetabolites that interfere with DNA replication and cell division, Undergoing radiation therapies.
Additional criteria may be found at this link: http://www.cdc.gov/breastfeeding/disease/.
A) Yes, the definition of breastfeeding does include both breastfeeding and the feeding of breast milk. These are both acceptable methods for inclusion in this measure.
21-item self-report measure used to screen for severity of depressive symptoms.
Contact information: The Psychological Corporation.
Tel: 800.228.0752
Web: www.psychcorp.com and http://www.pearsonassessments.com/HAIWEB/Cultures/en-us/Productdetail.htm?Pid=015-8018-370&Mode=summary
Self-report assessment screening for psychological problems in respondents across 9 symptom scales and 3 global indices; screens for specific symptoms as well as intensity.
Web: http://psychcorp.pearsonassessments.com/HAIWEB/Cultures/enus/Productdetail.htm?Pid=PAbsi
Non-standardized 20-item self-report measure assessing depressive symptoms.
Contact information: National Institute of Mental Health, Bethesda, MD 20892.
Web: www.nimh.nih.gov and http://counsellingresource.com/quizzes/cesd/index.html
Self-report assessment used to screen for major episodes of depression.
Contact information: World Health Organization.
Web: www.who.int/msa/cidi/ and http://www.ncbi.nlm.nih.gov/pubmed/9375257
42-item standardized self-report measure assessing caregiver mental health; 3 scales: Depression, Anxiety, and Stress.
Contact information: DASS Orders, PO Box 6780, UNSW Sydney NSW 1466, Australia.
Email: L.Camilleri@unsw.edu.au
Web: http://www2.psy.unsw.edu.au/groups/dass/order.htm
Additional information: Users may reproduce the scale without further permission providing they respect copyright by quoting the names of the authors, the title, and the source of the paper in all reproduced copies.
Web: http://www.dbpeds.org/articles/detail.cfm?TextID=485 (English)
9-item screener for DSM-IV depression criteria and other leading major depressive symptoms.
Web: http://www.phqscreeners.com/
35-item Likert-type response scale consisting of 7 domains to identify women who might be suffering from postpartum depression.
Contact information: Wester Psychological Services, 625 Alaska Avenue, Torrance, CA 90503 Tel: 800.648.8800
Web: http://www.wpspublish.com/store/p/2902/postpartum-depression-screening-scale-pdss
20-item self-administered survey to quantify the depressed status of a patient.
Web: https://psychology-tools.com/test/zung-depression-scale
If enrolled prenatally 3 months post birth.
If not enrolled prenatally 3 months post enrollment
NUMERATOR: For those not enrolled prenatally, number of primary caregivers enrolled in home visiting who are screened for depression within the first 3 months since enrollment; for those enrolled prenatally, the number of primary caregivers screened for depression within 3 months of delivery.
DENOMINATOR: For those not enrolled prenatally, the number of primary caregivers enrolled in home visiting for at least 3 months; for those enrolled prenatally, the number of primary caregivers enrolled in home visiting for at least three months post delivery.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: Caregivers currently receiving services are excluded from the calculation.
For reporting purposes Caregivers who do not have the measure completed in the data system are counted as not screened.
A) Yes, all Caregivers must be screened. They would be excluded from needed a referral if already receiving services.
A) The PHQ-9 scoring guide is as follows, 10 or above should select yes to a positive screen.
01-04: This is considered minimal depression, which suggests that the respondent may not need depression treatment.
05-09: This is considered mild depression.
10-14: This is considered moderate depression. – 10 or Above Should Select Yes to a Positive Screen in the Data System
15-19: This is considered moderately severe depression.
20-27: This is considered severe depression.
Starts: 3 Months Post Birth
Continues: 6, 9, 12, 15, 18, 21, 24*, 27, 30, 33 Months Post Birth
Continues: On the 3rd, 4th and 5th birthdays Post Birth
*NFP collection ends at 24 months post birth
NUMERATOR: Number of children (index child) enrolled in home visiting who received the last recommended well child visit based on the AAP schedule.
DENOMINATOR: Number of children (index child) enrolled in home visiting.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: N/A
A) Each time Measure 4 is being completed select all visits that have been completed that have not yet been marked as completed.
A) No, please select only the relevant completed visits. The visits displayed are based on the AAP schedule.
A) Caregiver self-report.
A) Well-child tele-health visits completed according to the AAP schedule can be included as meeting the criteria for Performance Measure 4. The AAP has issued guidance on providing well-child care vis telehealth during COVID-19. We recognize that not all providers may offer well-child visits, in person or via telehealth, during this time. AAP Guidance.
Only collected if the Caregiver enrolled prenatally or within 30 days after giving birth.
Collected at 8 weeks post birth of child.
NUMERATOR: Number of Caregivers enrolled in home visiting prenatally or within 30 days after delivery who received a postpartum visit with a healthcare provider within 8 weeks (56 days) of delivery.
DENOMINATOR: Number of Caregivers who enrolled in home visiting prenatally or within 30 days after delivery and remained enrolled for at least 8 weeks (56 days) after delivery.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: N/A
A) A postpartum visit is defined as a visit between the mother and her health care provider to assess her current physical health, including the status of pregnancy-related conditions like gestational diabetes, screen for postpartum depression, provide counseling on infant care and family planning as well as screening and referrals for the management of chronic conditions. Additionally, a provider may use this opportunity to conduct a breast exam and discuss breastfeeding.
The American College of Obstetricians and Gynecologists recommends that mothers receive a postpartum care visit 4 to 6 weeks after delivery. (Reference: Health Resources and Services Administration. Child Health USA 2013: Postpartum Visit and Well-Baby Care.)
A) Postpartum tele-health visits that meet the timeline criteria defined in the Performance Measure can be included as a completed visit. The American College of Obstetricians and Gynecologists recommends that women connect with their health care provider to discuss how their postpartum care visits may change during this time, including a shift to telemedicine or telehealth. ACOG Guidance.
3 Months Post Enrollment (Non NFP)
36 Weeks Gestation (NFP Only)
12 Months Post Birth (NFP Only)
NUMERATOR: Number of primary caregivers enrolled in home visiting who reported using tobacco or cigarettes enrollment and were referred to tobacco cessation counseling or services within 3 months of enrollment.
DENOMINATOR: Number of primary caregivers enrolled in home visiting who reported using tobacco or cigarettes at enrollment and were enrolled for at least 3 months.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: If the Caregiver is already receiving tobacco cessation services they are excluded from the calculation.
A) Combustibles (Cigars, Pipes, Hookahs, Bidis), Non-Combustibles (Chew, Dip, Snuff, Snus, Dissolvable), Electronic Nicotine Delivery Systems (ENDS).
A) Classes, support groups, hospitals, health insurance, talk to PCP.
A) Offering a referral counts as giving the referral, even if the client declines.
Non NFP
3, 6, 9, and 12 Months
NFP
0, 6, and 12 Months
NUMERATOR: Number of infants (index child aged less than 1 year) enrolled in home visiting whose primary caregiver reports that they are always placed to sleep on their backs, without bed-sharing and without soft bedding.
DENOMINATOR: Number of infants (index child) enrolled in home visiting who were aged less than 1 year during the reporting period.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: To be included in the Numerator the following responses need to be selected:
– Always places to sleep on back
– Never bed sharing
– Never soft bedding
A) Yes, follow your model(s) guidelines.
A) Sometimes to bed sharing.
A) Blankets, pillows, stuffed animals, or bumper pads.
3, 6, 9, 12, 15, 18, 21, 24, 27, 30, 33, 36 Months Post Enrollment.
Every 6 Months After 36 Months (3 Years), 42, 48, 54, 60, 66, 72, 78, 84 Months.
NUMERATOR: Number of parent-reported nonfatal injury-related visits to the ED during the reporting period among children (index child) enrolled in home visiting.
DENOMINATOR: Number of children (index child) enrolled in home visiting.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: The Numerator includes the number of reported injuries including if the same child has reported more than one injury related visit during the reporting period.
A) Injury-related emergency department visits are defined as injuries resulting from the following causes or mechanisms of injury: motor vehicle, suffocation, drowning, poisoning, fire/burns, falls, sports and recreation, and intentional injuries, such as child maltreatment. (Reference: Centers for Disease Control and Prevention. National Action Plan for Child Injury Prevention. 2012.)
A) No except if the ingestion resulted in poisoning.
Collected via administrative data from Office of Children, Youth and Families (OCYF).
NUMERATOR: Number of children (index child) enrolled in home visiting with at least 1 investigated case of maltreatment following enrollment within the reporting period.
DENOMINATOR: Number of children (index child) enrolled in home visiting.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: This is not collected within the Family Support Data System. This is reported using external data from the Office of Children, Youth, and Families (OCYF). OCDEL does not receive information about which individual children have investigated cases of maltreatment.
Healthy Family America’s proprietary tool, designed to promote attachment and positive interactions between parents and children. Observers score the following aspects of PCI on a seven-point scale: cues, holding and touching, expression, empathy, rhythm and reciprocity, and smiles. Training Required or Offered: Online training webinars followed by conversations with supervisors.
Nurse-Family Partnership’s proprietary tool outlines 18 caregiving behaviors that support children’s healthy growth and development, organized into four caregiving dimensions: Emotional Quality, Sensitivity and Responsivity, Support of Behavioral and Emotional Regulation, and Promotion of Develop-mental Growth.
Assesses four dimensions of parent behaviors (sensitivity, structuring, non-intrusiveness, and non-hostility) and two child behaviors (child responsiveness to adult, and child involvement of adult). Training Required or Offered: Developed and conducted by the International Center for Excellence in Emotional Avail-ability, is required.
Measures the quality and quantity of stimula-tion and support available to a child in the home environment. Includes 45 items organized into six subscales: parental responsivity, acceptance of child, organization of the environment, learning materials, parental involvement, and variety in experience. Administering the tool requires both observing and interviewing.
Uses a five-point scale to assess 12 key parenting behaviors, which fall into three categories: building relationships, promoting learning, and supporting confidence. Training Required or Offered: Online training and annual certi-fication required. Onsite training also available.
The Parent-Child Interaction Scales may be used to observe PCI in either a feeding or a teaching situ-ation. The scales measure both parenting behavior and child behavior. Subscales measure sensitivity, caregiver response to distress, caregiver’s social-emotional and cognitive growth fostering, and how responsive the child is to the caregiver’s behaviors. Training Required or Offered: Training is required and available from local instructors. Training to become a certified instructor is also available.
Comprises a checklist of 29 observable, develop-mentally supportive parenting behaviors in four do-mains: affection, responsiveness, encouragement, and teaching. The tool is also available in Spanish. Training Required or Offered: PICCOLO Training DVD includes 14 clips of PCI to help users practice observing and scoring.
Non-NFP
Collected on the child’s 1st, 2nd, 3rd, 4th, 5th, and 6th Birthdays Post Birth
NFP
3, 6*, 10, 17, 18* and 23 Months Post Birth
* As of January 1st, 2024 this measure will populate at 6 and 18 months for all children enrolled in NFP.
Based on model guidance the tools below should be completed at the following time periods:
– HOME – 6 and 18 Months Birth
– DANCE – 3, 10, 17, and 23 Months Post Birth
If the screening tool selected is not applicable to a time period populated, please select:
Not Screened, Too Old or Too Young for Screening Tool.
NUMERATOR: Number of primary caregivers enrolled in home visiting who receive an observation of caregiver-child interaction by the home visitor using a validated tool.
DENOMINATOR: Number of primary caregivers enrolled in home visiting with children reaching the target age range.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: The Child is excluded from the calculation if they were not within the valid age range for the selected tool within the reporting period.
If Measure 10 is not completed in the Family Support Data System they are counted in the denominator.
A) If the child is outside of the age range of the chosen tool the following should be selected:
Not Screened, Reason: Child too young or too old for screening tool.
Non-NFP
Start: 3 Months Post Enrollment
6, 9, 12, 15, 18, 21, 24, 27, 30, 33, 36 Months Post Enrollment
Every 6 Months After 36 Months (3 Years)
42, 48, 54, 60, 66, 72, 78, 84 Months
NFP
0, 6, 12, 18, and 24 Months Post Enrollment
NUMERATOR: Number of children (index child) enrolled in home visiting with a family member who reported that during a typical week s/he read, told stories, and/or sang songs with their child daily, every day.
DENOMINATOR: Number of children (index child) enrolled in home visiting.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: To be included in the Numerator 7 days must be selected.
A) Shared: The Caregiver should answer the question to the best of their ability based on what they understand to be occurring.
Lost Custody: Respond with 0 unless the answer is known by the Caregiver enrolled in the EBHV model.
A) Any Family Member who reads, sing songs, or tells stories to the Child during a typical week can be counted towards meeting the measure. It does not have to only be the Primary Caregiver.
30-item standardized caregiver-report measure assessing child development in the first 5 years; 5 domains: Communication, Gross Motor, Fine Motor, Problem-Solving, and Personal-Social.Squires, J., and Bricker, D. (2009). Ages and Stages Questionnaires: A parent-completed child monitoring system, third edition. Baltimore, MD: Paul Brookes.Contact: Brookes Publishing, 800.638.3775 https://www.brookespublishing.com/product/asq-3/
Non-NFP
9, 18, and 30 Months Post Birth
NFP
9 and 18 Months Post Birth
NUMERATOR: Number of children (index child) enrolled in home visiting with at least one screening within the AAP-defined age groups during the reporting period.
DENOMINATOR: Number of children (index child) enrolled in home visiting reaching the specified time frame during the reporting period.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: The Child is excluded if they have had a previous positive screen in a prior reporting period or if they are currently receiving services prior to enrollment.
A) Programs may choose to screen at additional ages but are expected to report on screenings at the AAP-recommended ages. If models require or programs choose to screen at additional ages beyond the AAP recommendations, only data about screenings based on the AAP recommendations should be reported.
A) This is not a required screening at this time. However, it may be required by your model.
A) The system does not take this into account in the calculation. Programs should follow the implementation instructions for the ASQ. The ASQ provides guidance on adjusting for premature birth.
ASQ developer guidelines: Adjust a child’s age only if he or she is 3 or more weeks premature. This means a child born at or before 36 weeks should have his or her age-adjusted. Age should only be adjusted for children under age 2. Once a child is 2 or older, prematurity no longer needs to be considered and the actual age should be used. The ASQ developers provide an online calculator to determine which assessment to use: https://agesandstages.com/free-resources/asq-calculator/.
Using the calculator if a Baby was Born on November 9th, 2019 on August 9th, 2019 they would be 9 months of age (but they were born 4 weeks premature) so it says to use the 8 month ASQ for the 9-month screening.
Measure 12 is following the American Academy of Pediatrics (AAP) recommended screening protocols: The AAP recommends conducting developmental surveillance at every health supervision visit and conducting general developmental screening using evidence-based tools at 9, 18, and 30 months, or whenever a concern is expressed.
A) A child may be excluded from the screening if they have a previously identified developmental delay (prior to enrollment or prior to reaching an age-recommended screening).
Every home visit is documented (prenatal and postpartum)
Prenatal Home Visits
Not required to ask M13 Question
Postpartum Home Visits
Required to ask M13 Question
NUMERATOR: Number of postnatal home visits where primary caregivers enrolled in home visiting were asked if they have any concerns regarding their child’s development, behavior, or learning.
DENOMINATOR: Total number of postnatal home visits during the reporting period.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: N/A
A) There are no age restrictions for collecting data on behavioral concerns. This question should be asked at all postnatal home visits regardless of the index child’s age.
A) Select the Telehealth / Virtual home visiting option when completing this measure. Only enter the visit if this is considered a completed visit per the EBHV model being implemented. Please note that Texting does not count as a visit.
A) Yes, if the Telehealth or virtual visit is approved by the EBHV model and counts as an approved model visit (excludes texting).
A) This should not be counted a pre-natal visit, select no and answer the behavioral concerns question regarding the enrolled child.
A) The Measure 13 Home Visits are entered for ever home visit as defined by the model. If the model considers each child to have a visit then two home visits should be entered for that day.
– Severity of Violence Against Women Scale (SVAWS)
– Domestic Violence Evaluation (DOVE)
5-question screen involving open-ended questions to assess intimate partner violence.
Deshpande, N.A. and Lewis-O’Connor, A. (2013). Screening for intimate partner violence during
pregnancy. Reviews in Obstetrics and Gynecology, 6:141-148.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4002190/figure/F5/
30-item scale completed by male batterer that measures the frequency of perpetration of physical
and psychological abusive behaviors.
Shepard, M. F., and Campbell, J. A. (1992). The Abusive Behavior Inventory: a measure of
psychological and physical abuse. Journal of Interpersonal Violence, 7: 291–305.
Contact: Sage Publications. Used with permission.
http://www.cdc.gov/ncipc/dvp/Compendium/IPV%20Compendium.pdf
30-item assessment of partner abuse across 4 subscales: Severe Combined Abuse, Emotional Abuse, Physical Abuse, and Harassment.
Hegarty K., Sheehan M., and Schonfeld C. (1999). A multidimensional definition of partner abuse:
development and preliminary validation of the Composite Abuse Scale. Journal of Family
Violence, 14: 399–415.
Hegarty K., Bush R., and Sheehan M. (2005). The Composite Abuse Scale: further development and assessment of reliability and validity of a multidimensional partner abuse measure in clinical
settings. Violence and Victims, 20: 529-547.
Contact: Marilyn Ford-Gilboe, mfordg@uwo.ca
bmjopen-2016-012824supp.pdf
78-item non-standardized; administered as either self-report or observational measure to assess
domestic violence, specific to partner relationship; 3 subscales: Physical Aggression,
Psychological Aggression, and Sexual Coercion.
Straus, M. A., Hamby, S. L., Boney-McCoy, S., Sugarman, D. B. (1996). The Revised Conflict Tactics
Scale (CTS2): development and preliminary psychometric data. Journal of Family Issues, 17: 283–
316.
Contact: Western Psychological Services, 800.648.8857
https://www.wpspublish.com/store/p/2728/cts-conflict-tactics-scales
6-item screen to identify patients experiencing domestic violence during well-child pediatric visits.
Siegel, R.M., Hill, T.D., Henderson, V.A., Ernst, H.M., and Boat, B.W. (1999). Screening for domestic violence in the community pediatric setting. Pediatrics, 104: 874-77.
http://www.cdc.gov/violenceprevention/pdf/ipv/ipvandsvscreening.pdf
45-item self-report measure; 2 scales: OFTEN and DISTRESS scales measure how often a harassing Form 2 Performance Indicators and Systems Outcomes Toolkit 93 September 2018
behavior occurs and how distressing the behavior is perceived by the participant.
Sheridan, D. J. (2001). Treating survivors of intimate partner abuse: forensic identification and
documentation. In: Olshaker JS, Jackson MC, Smock WS, editors. Forensic emergency medicine.
Philadelphia, PA: Lippincott, Williams, & Wilkins, 203–228.
http://www.cdc.gov/ncipc/dvp/Compendium/IPV%20Compendium.pdf
4-question assessment to reliably identify women experiencing IPV who present in clinical settings.
Sohal, H., Eldridge, S., and Feder, G. (2007). The sensitivity and specificity of four questions (HARK) to identify intimate partner violence: A diagnostic accuracy study in general practice. BMC
Family Practice, 8, 49.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2034562/table/T1/
4-question assessment to reliably identify women experiencing IPV who present in clinical settings.
Sohal, H., Eldridge, S., and Feder, G. (2007). The sensitivity and specificity of four questions (HARK) to identify intimate partner violence: A diagnostic accuracy study in general practice. BMC
Family Practice, 8, 49.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2034562/table/T1/
4-question assessment asking how often a partner hurts you, insults you, threatens you, and
screams at you to form the acronym HITS.
Deshpande, N.A. and Lewis-O’Connor, A. (2013). Screening for intimate partner violence during
pregnancy. Reviews in Obstetrics and Gynecology, 6:141-148.
Sherin, K.M., Sinacore, J.M., Li, X.Q., et al. (1998). HITS: a short domestic screening tool for use in a family practice setting. Family Medicine, 30:508–512.
http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4002190/figure/F4/
5 items adapted from the Abuse Assessment Screen (AAS) to assess ongoing physical, sexual,
emotional IPV, and fear.
Ernst, A.A., Weiss, S.J., Cham, E., and Marquez, M. (2002). Comparison of three instruments for
assessing ongoing intimate partner violence. Medical Science Monitor, (8)3, 197-201.
Weiss, S.J., Ernst, A.A., Cham, E., and Nick, T.G. (2003). Development of a screen for ongoing
intimate partner violence. Violence and Victims, (18)2, 131-141.
https://www.cdc.gov/violenceprevention/pdf/ipv/ipvandsvscreening.pdf
3-question short screening tool for interpersonal violence.
Koziol-McLain, J., Brand, D., Morgan, D., Leff, M., and Lowenstein, S. R. (2000). Measuring injury risk factors: Question reliability in a statewide sample. Injury Prevention, 6, 148-150.
Koziol-McLain, J., Coates, C. J., and Lowenstein, S. R. (2001). Predictive validity of a screen for
partner violence against women. American Journal of Preventive Medicine, 21(2), 93-100.
Contact: Jane Koziol-McLain, jane.koziol-mclain@aut.ac.nz
21-item self-report measure of psychological abuse; 4 subscales: Jealous Control, Ignore, Ridicule
Traits, and Criticize Behavior.
Sackett, L. A., and Saunders, D. G. (1999). The impact of different forms of psychological abuse on
battered women. Violence and Victims, 14:105–177.
http://www.midss.org/content/profile-psychological-abuse-women
10-item measure of psychological/emotional victimization.
Smith, P., Earp, J., and DeVellis, R. (1995). Measuring battering: development of the Women’s
Experiences with Battering (WEB) Scale. Women’s Health: Research on Gender, Behavior, and
Policy, 1:273–288.
Smith, P., Smith, J., and Earp, J. (1999). Beyond the measurement trap: a reconstructed
conceptualized and measurement of woman battering. Psychology of Women Quarterly,
23:177–193.
Smith, P., Thornton, G., DeVellis, R., Earp, J., and Coker, A. (2002). A population-based study of the prevalence and distinctiveness of battering, physical assault, and sexual assault in intimate
relationships. Violence Against Women, 8:1208–1232.
Contact: Futures Without Violence, 415.678.5500, info@futureswithoutviolence.org
https://www.dropbox.com/s/53yhktumby1nd9k/RAT%20English%20Spanish.pdf?dl=0
4-items asking about problems occurring in the household using a picture scale to rate responses.
Wasson, J.H., Jette, A.M., Anderson, J., Johnson, D.J., Nelson, E.C., and Kilo, C.M. (2000). Routine,single-item screening to identify abusive relationships in women. The Journal of Family Practice, 49: 1017-22.
http://www.cdc.gov/violenceprevention/pdf/ipv/ipvandsvscreening.pdf
6-question screening protocol administered by a clinician or self-report to identify relationship
abuse. Heron, S.L., Thompson, M.P., Jackson, E., and Kaslow, N.J. (2003). Do responses to an intimate partner violence screen predict scores on a comprehensive measure of intimate partner
violence in low-income black women? Annals of Emergency Medicine, 42: 483-91.
http://www.cdc.gov/violenceprevention/pdf/ipv/ipvandsvscreening.pdf
8-question screener to identify women who are victims of abuse.
Brown, J.B., Lent, B., Schmit, G., and Sas, G. (2000). Application of the Woman Abuse Screening Tool (WAST) and WAST-Short in the family practice setting. Journal of Family Practice, 49:896-903.
http://womanabuse.webcanvas.ca/documents/wast.pdf
6 Months Post Enrollment.
NUMERATOR: Number of primary caregivers enrolled in home visiting who are screened for IPV using a validated tool within 6 months of enrollment.
DENOMINATOR: Number of primary caregivers enrolled in home visiting for at least 6 months.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: All primary caregivers should be screened regardless of relationship status.
Caregivers who have a Measure 14 that was not completed in the reporting period are still included in the Denominator.
A) Yes, all primary caregivers should be screened for IPV regardless of relationship status while enrolled in an Evidence-Based Home Visiting model.
IPV refers to physical violence, sexual violence, stalking, and psychological aggression (including coercive acts) by a current or former intimate partner. An intimate partner is a person with whom one has a close personal relationship that can be characterized by the following: emotional connectedness, regular contact, ongoing physical contact and sexual behavior, identity as a couple, and familiarity and knowledge about each other’s lives. (Reference: Centers for Disease Control and Prevention. Injury Prevention and Control: Division of Violence Prevention, 2015.).
A) The tool NFP uses includes all of the same questions as the HITS screening tool. NFP providers should select the HITS.
Collected via demographics, at entry, update, or at exit. Only collected if caregiver does not already have a high school diploma, equivalent such as a GED, or a higher degree.
NUMERATOR: Number of primary caregivers who enrolled in or maintained continuous enrollment in middle school or high school, or completed a high school degree or equivalent after enrollment in home visiting (and met the conditions specified in the denominator).
DENOMINATOR: Number of primary caregivers without a high school degree or equivalent at enrollment.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: N/A
A) This behavior is as expected. Update will generate a new measure 15 while edit will display the previously entered measure 15. If it is showing what they entered on edit, then the information saved correctly.
All EBHV
6 Months Post Enrollment
6, 12, 18, 24, 30, 36 Months Post Enrollment
NUMERATOR: Number of primary caregivers enrolled in home visiting who reported having continuous health insurance coverage for the most recent 6 consecutive months at the most recent data collection time point in the reporting period.
DENOMINATOR: Number of primary caregivers enrolled in home visiting for at least 6 months.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: Caregiver must be enrolled for at least 6 months to be included in the denominator.
A) Continuous health insurance coverage refers to having coverage without any lapses.
Only Collected If Caregiver Screens Positive
If Enrolled Prenatally
6 Months Post Birth
If Not Enrolled Prenatally
6 Months Post Enrollment
If Caregiver Does Not Receive a Service They Need To Be Re-screened Until They:
1. No Longer Screen Positive
2. Receive a Service
NUMERATOR: Number of primary caregivers enrolled in home visiting who received recommended services for depression (and met the conditions specified in the denominator).
DENOMINATOR: Number of primary caregivers enrolled in home visiting who had a positive screen for depression within 3 months of enrollment (for those not enrolled prenatally) or within 3 months of delivery (for those enrolled prenatally) and were referred for services.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: If Measure 17 is not completed in the data system during the reporting period the Caregiver is counted in the Denominator as not receiving services.
Caregiver is excluded from the calculation if the Caregiver is already receiving services after screening.
A) For those participants who screen positive for depressive symptoms but are already receiving services for depression, you do not need to provide a referral.
A) Appointment with a therapist, appointment with a psychiatrist, meeting with a mental health consultant, follow up with primary care physician, follow up with OBGYN, inpatient psychiatric hospitalization, support groups.
A) No, calling the Maternal Health Hotline is not considered a considered a completed depression referral for PM 17. The National Maternal Mental Health Hotline provides free confidential support, resources, and referrals to pregnant and postpartum individuals facing mental health challenges and their loved ones, which may or may not result in the caller receiving services for depression that meet HRSA guidance (i.e., specific techniques and intervention models delivered in the context of client characteristics, culture, and preferences that have shown to have positive effects on outcomes through rigorous evaluations and have demonstrated to achieve positive outcomes for the client). If disclosed by the participant to the home visitor, awardees may be able to track completion of referral services recommended by the hotline and determine inclusion for reporting in accordance with HRSA guidance.
Only collected if Child Scores Below The Cutoff
12 Months Post Birth
21 Months Post Birth*
33 Months Post Birth
*NFP
Ends at 21 Months Post Birth
NUMERATOR: Number of children enrolled in home visiting who a) received individualized developmental support from a home visitor; b) were referred to early intervention services and receive an evaluation within 45 days; OR c) were referred to other community services who received services within 30 days (and met the condition specified in the denominator).
DENOMINATOR: Number of children enrolled in home visiting with positive screens for developmental delays (measured using a validated tool).
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: If Measure 18 is not completed in the data system during the reporting period the Child is counted in the Denominator as not receiving services.
The Child is excluded from the calculation if the Child has a previously identified developmental delay or are already receiving services prior to enrollment.
Collected only if Caregiver Screens Positive for IPV at:
9 Months Post Enrollment
NUMERATOR: Number of primary caregivers enrolled in home visiting who received referral information to IPV resources (and met the conditions specified in the denominator).
DENOMINATOR: Number of primary caregivers enrolled in home visiting with positive screens for IPV (measured using a validated tool) within 6 months of enrollment.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: If Measure 19 is not completed in the data system during the reporting period the Caregiver is counted in the Denominator as not referred to services.
3-item screening instrument for identifying hazardous drinking or active alcohol use disorders.
Bradley, K. A., Bush, K. R., Epler, A. J., Dobie, D. J., Davis, T. M., Sporleder, J. L., Maynard, C.,
Burman, M. L., & Kivlahan, D. R. (2003). Two Brief Alcohol-Screening Tests From the Alcohol Use Disorders Identification Test (AUDIT): Validation in a Female Veterans Affairs Patient Population. Archives of Internal Medicine, 163(7), 821–829. https://doiorg.ezproxyhhs.nihlibrary.nih.gov/10.1001/archinte.163.7.82
Bush K, Kivlahan DR, McDonell MB, et al (1998). The AUDIT alcohol consumption questions
(AUDIT-C): an effective brief screening test for problem drinking. Ambulatory Care
Quality Improvement Project (ACQUIP). Archives of Internal Medicine. 158 (16):1789-95. https://doi.org/10.1001/archinte.158.16.1789
Frank, D., DeBenedetti, A.F., Volk, R.J. et al. (2008). Effectiveness of the AUDIT-C as a Screening
Test for Alcohol Misuse in Three Race/Ethnic Groups. Journal of General Internal Medicine 23(6), 781–787. https://doi.org/10.1007/s11606-008-0594-0
https://cde.drugabuse.gov/instrument/f229c68a-67ce-9a58-e040-bb89ad432be4
10-item self-report measure for identifying hazardous drinking or active alcohol use disorders.
Bradley, K. A., Bush, K. R., Epler, A. J., Dobie, D. J., Davis, T. M., Sporleder, J. L., Maynard, C.,
Burman, M. L., & Kivlahan, D. R. (2003). Two Brief Alcohol-Screening Tests From the Alcohol Use Disorders Identification Test (AUDIT): Validation in a Female Veterans Affairs Patient Population. Archives of Internal Medicine, 163(7), 821–829. https://doiorg.ezproxyhhs.nihlibrary.nih.gov/10.1001/archinte.163.7.82
Steinbauer, J. R., Cantor, S. B., Holzer III, C. E., & Volk, R. J. (1998). Ethnic and sex bias in primary care screening tests for alcohol use disorders. Annals of Internal Medicine, 129(5), 353–362. https://doi.org/10.7326/0003-4819-129-5-199809010-00002
https://cde.drugabuse.gov/instrument/f3552f38-6bf7-1ae1-e040-bb89ad432ee3
8-item questionnaire developed by the World Health Organization (WHO) assessing frequency of substance use and related problems. WHO ASSIST Working Group (2002). The Alcohol, Smoking and Substance Involvement Screening Test (ASSIST): development, reliability and feasibility. Addiction (Abingdon, England), 97(9), 1183–1194. https://doi-org.ezproxyhhs.nihlibrary.nih.gov/10.1046/j.1360-0443.2002.00185.x
Humeniuk, R., Ali, R., Babor, T. F., Farrell, M., Formigoni, M. L., Jittiwutikarn, J., de Lacerda, R. B., Ling, W., Marsden, J., Monteiro, M., Nhiwatiwa, S., Pal, H., Poznyak, V., & Simon, S. (2008). Validation of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). Addiction (Abingdon, England), 103(6), 1039–1047. https://doi-org.ezproxyhhs.nihlibrary.nih.gov/10.1111/j.1360-0443.2007.02114.x
https://www.who.int/publications/i/item/978924159938-2
2-item version of the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST). The ASSIST-FC includes one question on frequency of current use and a second question regarding concern expressed by a friend, relative, or others.
McRee, B., Babor, T. F., Lynch, M. L., & Vendetti, J. A. (2018). Reliability and Validity of a Two-Question Version of the World Health Organization’s Alcohol, Smoking and Substance Involvement Screening Test: The ASSIST-FC. Journal of Studies on Alcohol and Drugs, 79(4), 649–657.
https://doi.org/10.15288/jsad.2018.79.649
4-item questionnaire for alcohol and drug problems. The CAGE-AID screener focuses on lifetime use.
Brown, R. L., & Rounds, L. A. (1995). Conjoint screening questionnaires for alcohol and other drug abuse: criterion validity in a primary care practice. Wisconsin medical journal, 94(3), 135–140.
https://www.hiv.uw.edu/page/substance-use/cage-aid
10-item self-report to assess involvement with drugs, excluding alcohol, and drug-related problems.
Skinner, H. A. (1982). The drug abuse screening test. Addictive Behaviors, 7(4), 363–371.
https://doi-org.ezproxyhhs.nihlibrary.nih.gov/10.1016/0306-4603(82)90005-3
Yudko, E., Lozhkina, O., & Fouts, A. (2007). A comprehensive review of the psychometric properties of the Drug Abuse Screening Test. Journal of Substance Abuse Treatment, 32(2), 189–198. https://doi.org/10.1016/j.jsat.2006.08.002
https://cde.drugabuse.gov/instrument/e9053390-ee9c-9140-e040-bb89ad433d69
Tool consisting of a single question screening for substance use in 4 category types (alcohol, tobacco products, prescription drugs for non-medical reasons, illegal drugs) for adults.
https://archives.drugabuse.gov/publications/resource-guide-screening-drug-use-in-general-medical-settings/nida-quick-screen
5-question screen for alcohol, tobacco, marijuana, and illicit drug use developed for obstetrical patients.
Chasnoff, I. J., Wells, A.M., McGourty, R. ., & Bailey, L.K. (2007). Validation of the 4P’s
Plus© screen for substance use in pregnancy validation of the 4P’s Plus. Journal of Perinatology, 27(12), 744–748. https://doi.org/10.1038/sj.jp.7211823
https://www.ntiupstream.com/4psabout
4-item questionnaire originally developed to screen for risk drinking among pregnant individuals.
Sokol, R. J., Martier, S. S., & Ager, J. W. (1989). The T-ACE questions: practical prenatal of risk-drinking. American Journal of Obstetrics and Gynecology, 160(4), 863–870.
https://doi.org/10.1016/0002-9378(89)90302-5
5-item tool originally developed to screen for risk drinking during pregnancy. Russell, M. (1994). New Assessment Tools for Risk Drinking During Pregnancy: T-ACE, TWEAK, and Others. Alcohol Health and Research World, 18(1), 55–61.
https://pubs.niaaa.nih.gov/publications/assessingalcohol/instrumentpdfs/74_tweak.pdf
6-item tool developed to identify risk for abuse and dependency for alcohol and other drugs.
https://ncsacw.acf.hhs.gov/files/TrainingPackage/MOD2/ExampleScreenQuestionsUNCOPE.pdf
https://arise-network.com/wp-content/uploads/2017/08/UNCOPEforconcernedothersScreening.pdf
6 months post enrollment.
NUMERATOR: Number of primary caregivers enrolled in home visiting who were screened for both unhealthy alcohol use and drug use using validated tool(s) within 6 months of enrollment.
DENOMINATOR: Number of primary caregivers enrolled in home visiting for at least 6 months.
CALCULATION: = Numerator / Denominator
CLARIFICATIONS: N/A
A) This measure is optional for all EBHV programs. OCDEL has made this measure optional for all EBHV programs, it may be required in the future.
At this time, HRSA, our federal funder, has not made any determinations on whether these will be required in the future and intends to evaluate feedback from both the optional reporting measures to inform any future updates to data collection activities related to substance use screening and referrals.
A) The definition of unhealthy alcohol and drug use should align with the validated substance use screening tool’s definition.
A) Yes, if the chosen tool or tool(s) do not address both drugs and alcohol you will need to complete a minimum of two tools with the Caregiver to meet the requirements of this measure.
A) No, this will display for all primary Caregivers at 6 months post enrollment, if their 6 month post enrollment date is after 10/1/2021. If it is displaying for a Caregiver that has a 6 month post enrollment date prior to 10/1/2021 please update the Caregiver so the measure is removed.
Staff should select that they are not completing the measure by selecting the following options in the image below.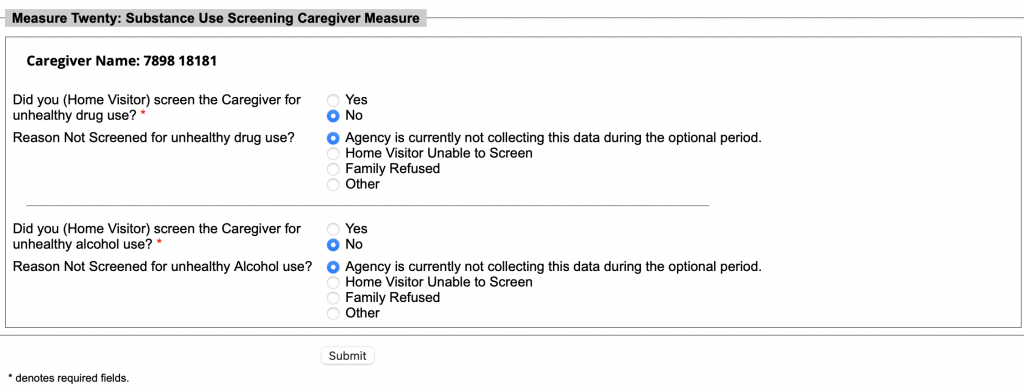
9 Months Post Enrollment
NUMERATOR: Number of primary caregivers enrolled in home visiting who received recommended services for substance use (and met the conditions specified in the denominator).
DENOMINATOR: Number of primary caregivers enrolled in home visiting who had a positive screen for unhealthy alcohol use and/or drug use (measured using a validated tool) within 6 months of enrollment and were referred for services.
CLARIFICATIONS: N/A
A) Specific techniques and intervention models delivered in the context of client characteristics, culture, and preferences that have shown to have positive effects on outcomes through rigorous evaluations and have demonstrated to achieve positive outcomes for the Caregiver.
Programatic Reports
Funded Slot / Goals Change Request
Users with access: The Agency Administrator and Agency Data Users have access to this feature. 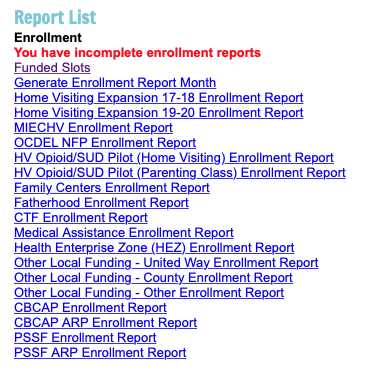

County: Will only display those counties currently linked to your agency. Please email your Family Support Consultant and the Data System RA account to add additional counties if needed.
Funded Slots / Goals: Please do not switch from one to the other as this will be rejected as certain programs are required to be reported on in certain ways. 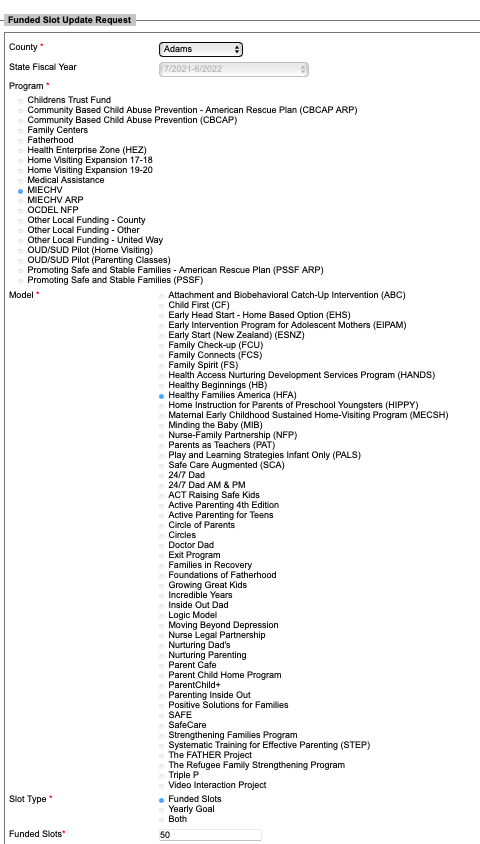
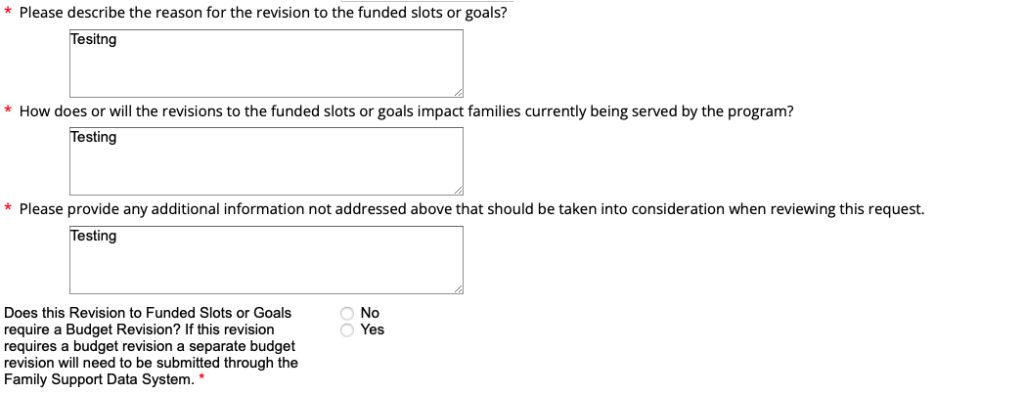
Enrollment Report
Updated Enrollment Report Generation Process as of August 10th, 2022
The Agency shall generate a monthly enrollment report using the data system no later than the 15th of each month for the previous month’s enrollment. As an example: the report for the month of October would be generated in November by November 15th.
The Agency shall review the enrollment report for accuracy by no later than the 15th of each month for the previous month’s enrollment.
If the report is incorrect the Agency shall edit the report and provide an explanation for the edit.
The Agency may add comments as necessary to explain current enrollment trends and additional information relevant to enrollment.
The Agency as appropriate shall notify the Department of any inconsistencies with the enrollment report.
The data system will prompt the enrollment report to be generated starting the 15th of each month for the previous month’s enrollment to ensure that the reports are being generated.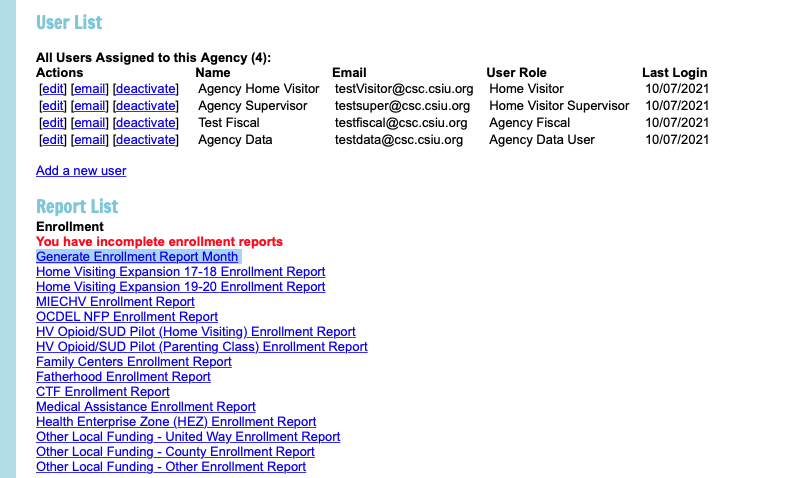
The oldest report by month must be generated first.
Please do not generate enrollment reports out of order
Generate starting with: July to June or October to September depending on the year your program is operating on. 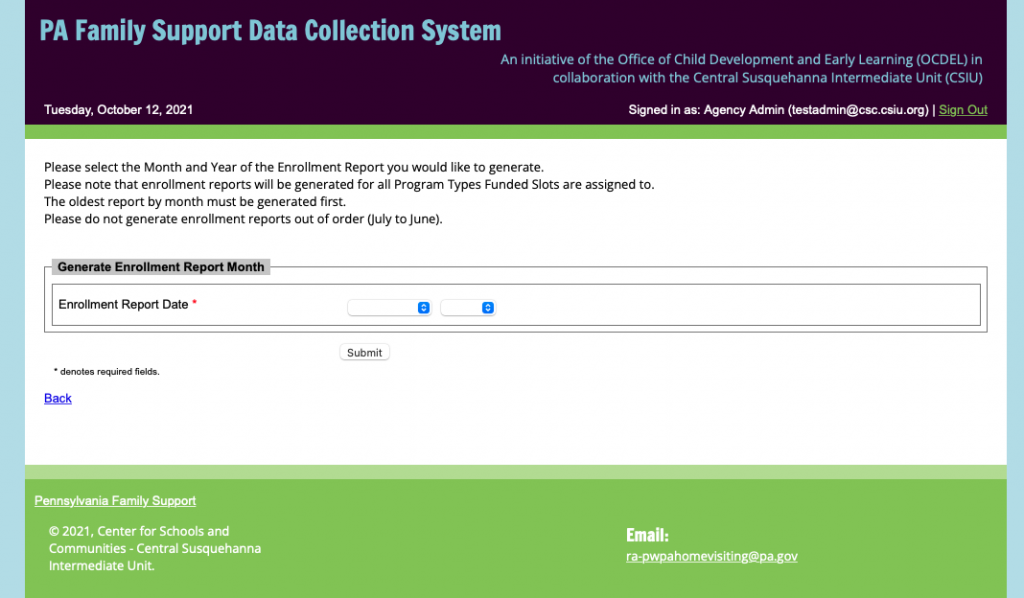
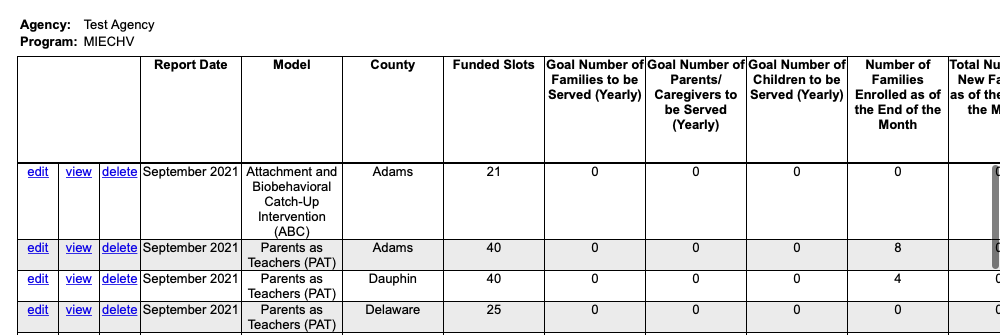
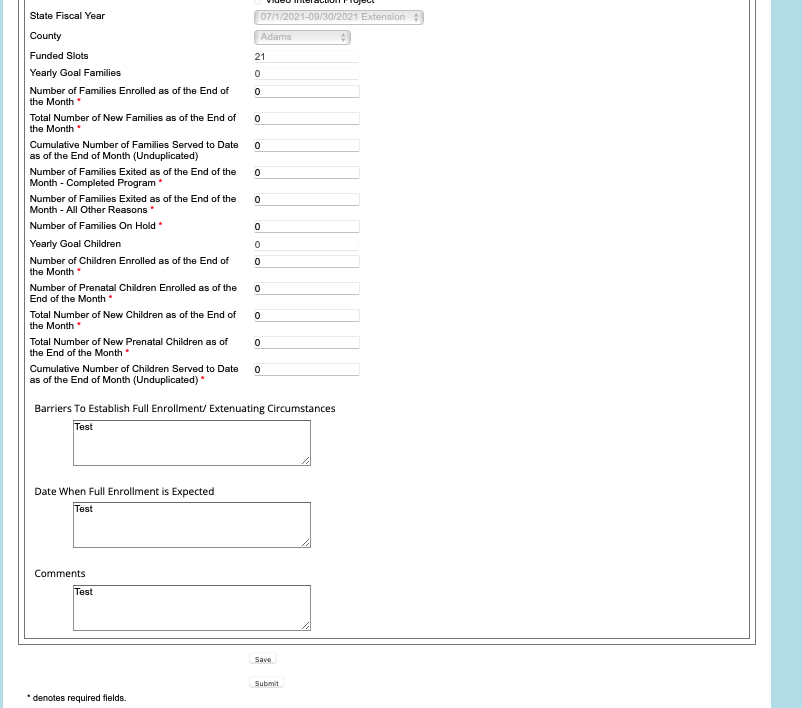
Once edits are submitted the report will need to be unlocked by the agencies designated Family Support Consultant or the RA Account.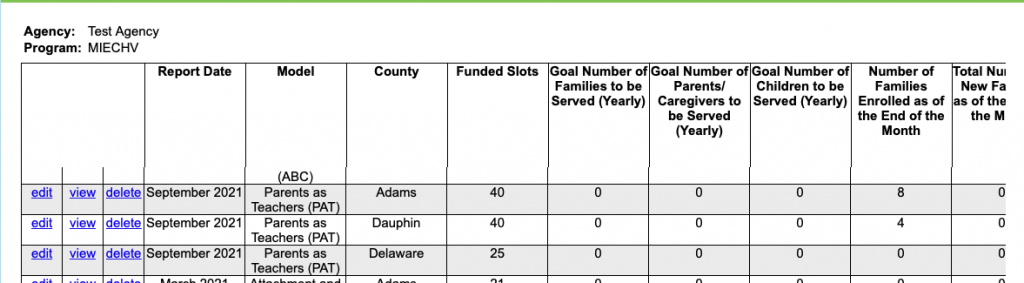
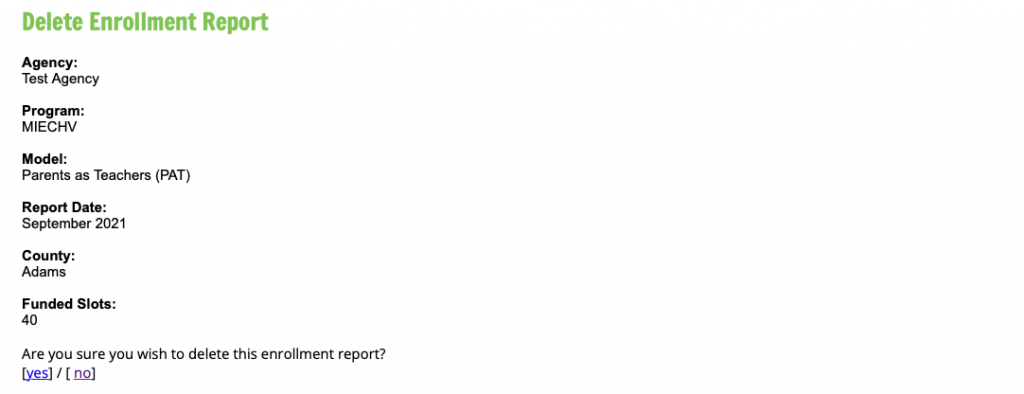
A) The Agency Administrator, Data User and Supervisor roles may delete reports prior to submission. 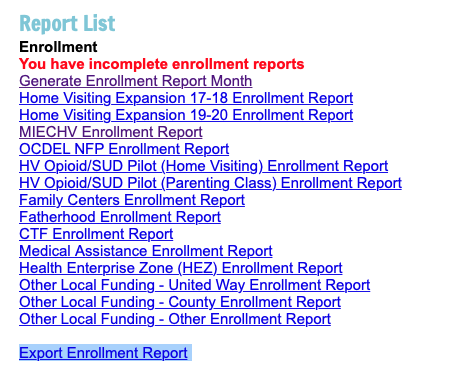
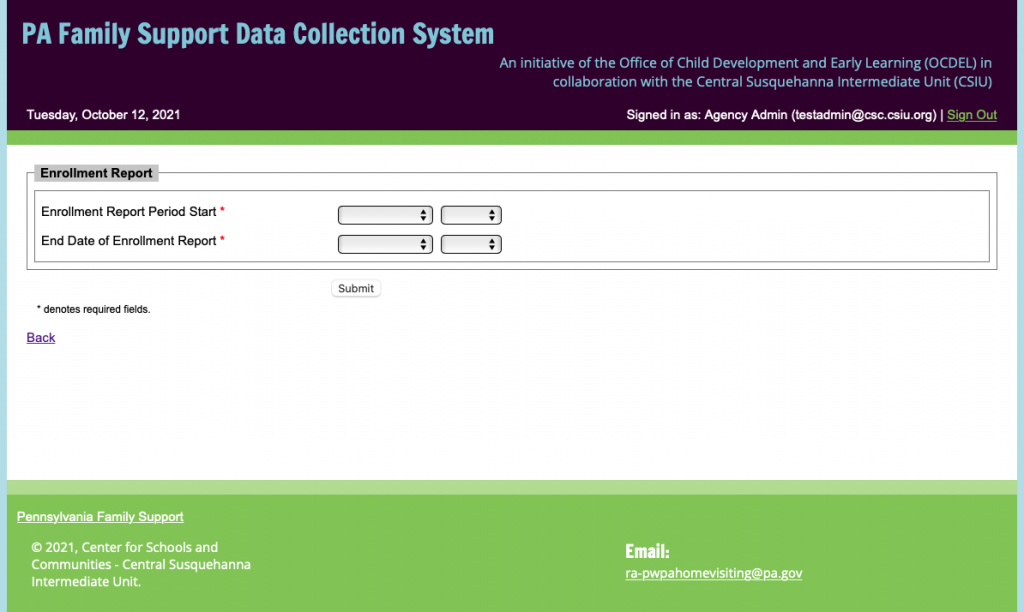
Example: 10 families were enrolled in September, in October 5 new families enrolled. When the report for October is generated in November the cumulative number for October should be 15 families.
Example: 10 children were enrolled in September, in October 5 new children enrolled. When the report for October is generated in November the cumulative number for October should be 15 children.
Staffing Report
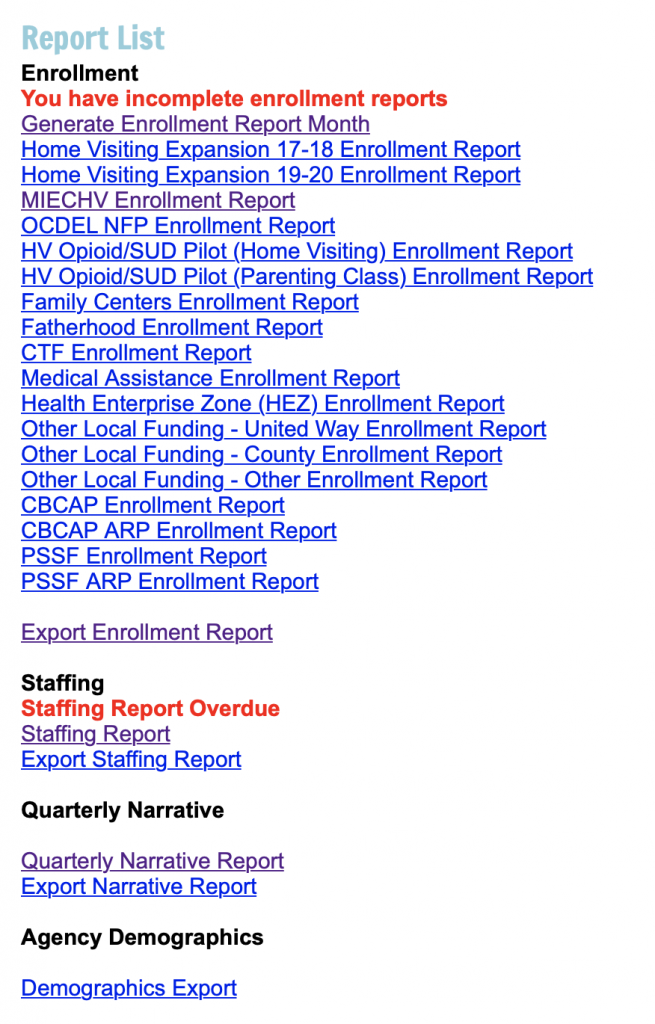
FTE Reporting Notes: If you choose Children’s Trust Fund (CTF), Fatherhood (PRF), Medical Assistance (MA), Other Local Funding (County, Other, United Way), or OUD/SUD Pilot (Parenting Classes) you DO NOT need to submit the FTE fields at this time.
FTE Reporting Notes: If you choose Family Centers (FC), Home Visiting Expansion (HVE), OCDEL NFP, or OUD/SUD Pilot (Home Visiting) you DO need to submit the FTE fields at this time.
MIECHV Reporting Notes: If MIECHV is chosen you will also report data separated by EBHV Model. 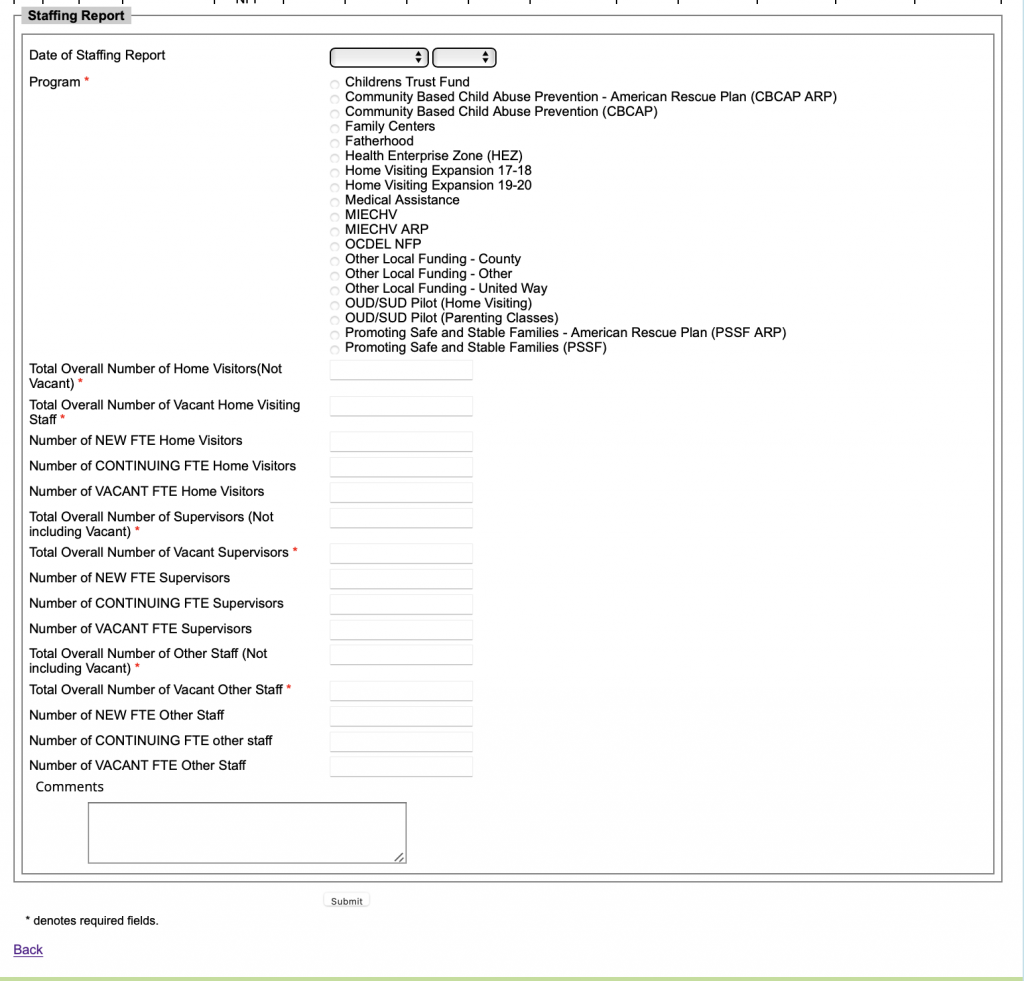
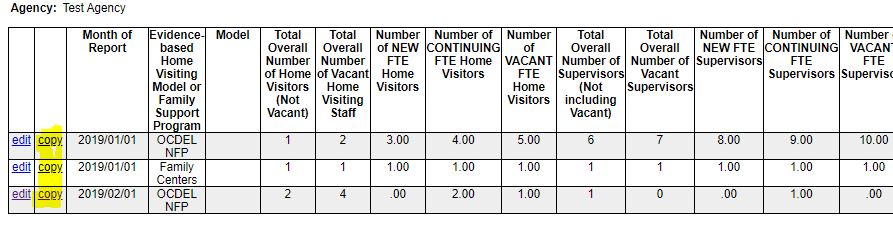
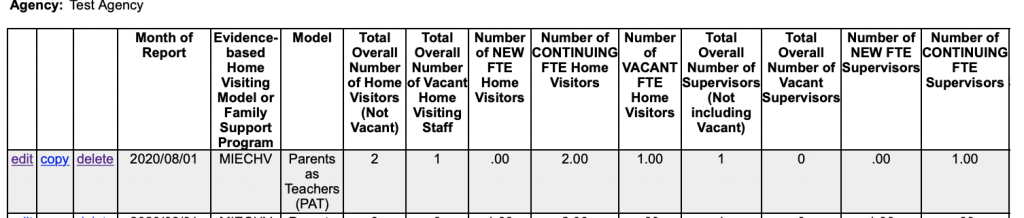
Home Visitor/Supervisor/Other Staff: A FTE home visitor(s)/supervisor(s)/other staff who begins employment with your agency during the reporting period. Only report the proportion of the FTE that is supported by the Program Type.
Home Visitor/Supervisor/Other Staff: A FTE home visitor(s)/supervisor(s)/other staff who was employed by your agency during the previous reporting period and continued employment. Only report the proportion of the FTE that is supported by grant funds.
Home Visitor/Supervisor/Other Staff: A position that is funded by grant funds but does not have a home visitor/supervisor/other staff filling the position. Only report the proportion of the FTE that is supported by grant funds.
For example, a 1.0 FTE staff member who is supported at 30% through MIECHV grant funds and 70% through expansion would be reported as 0.3 FTE in MIECHV and .70 FTE in Expansion.
Quarterly Narrative Report
Please save as you complete each section using the save option at the bottom of the screen. ![]()

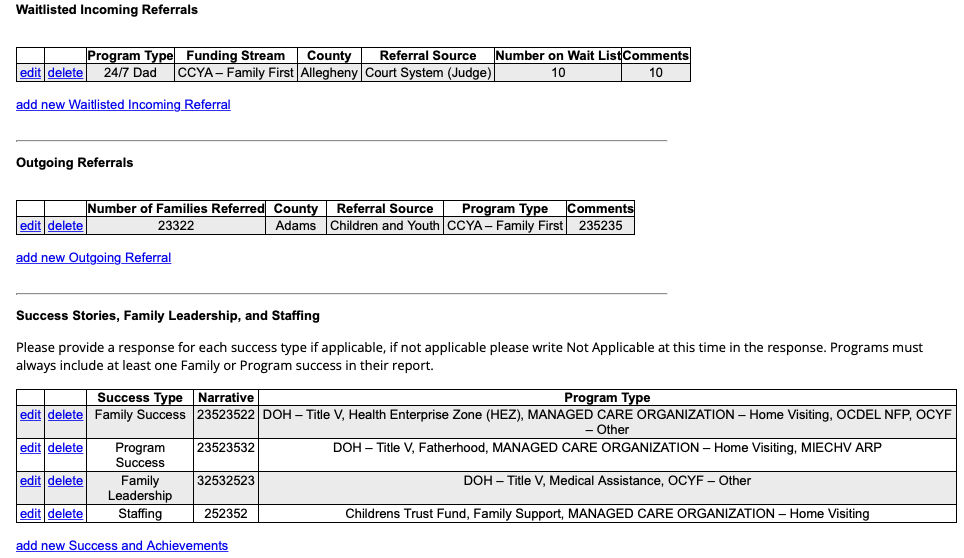
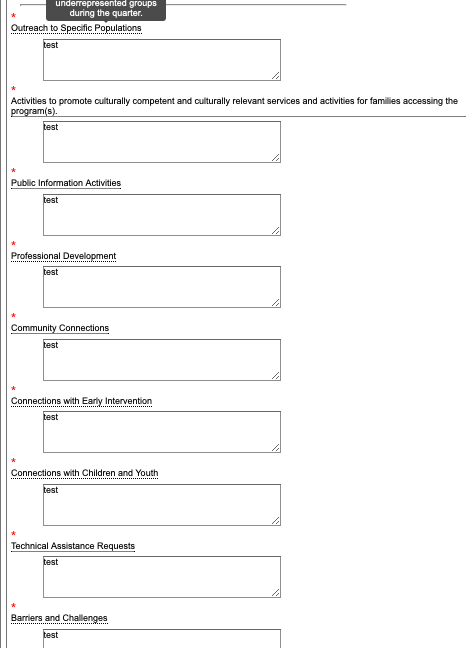
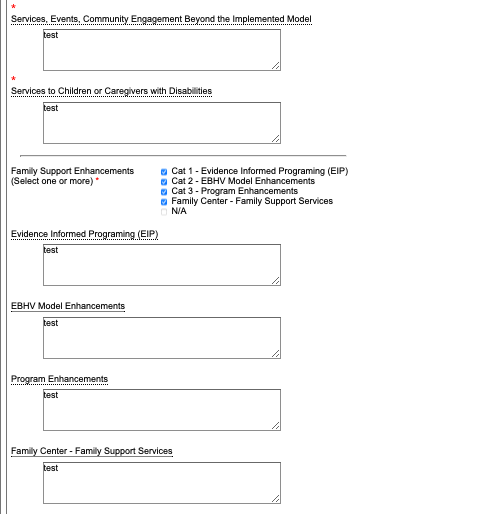
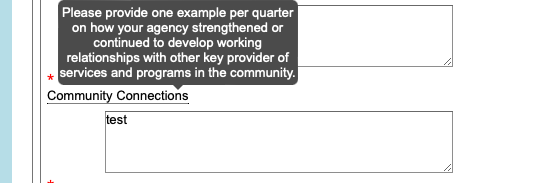
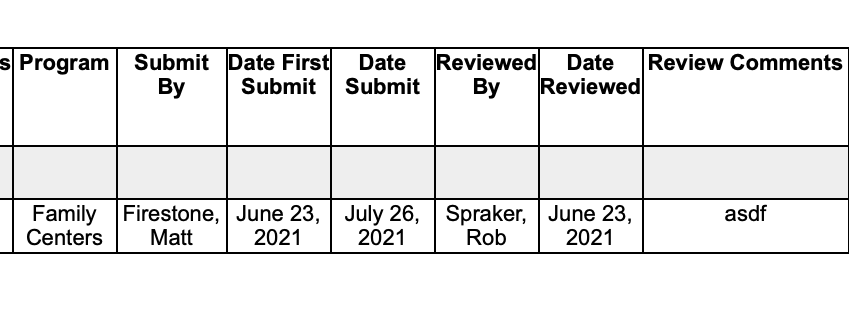
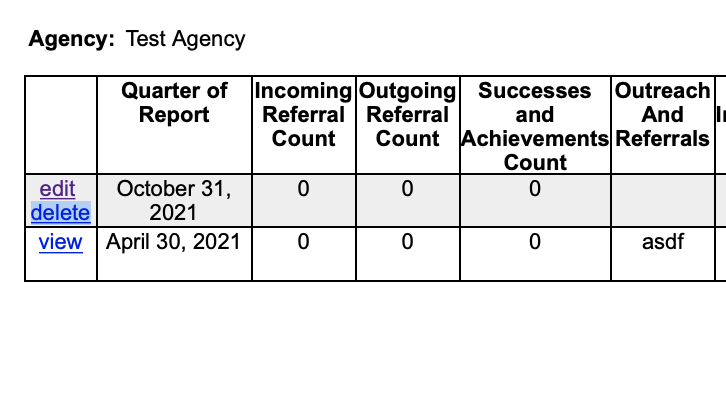
Report Due Dates
Quarterly Breakdown
Quarter State Fiscal Year
July to JuneFederal Fiscal Year
October to SeptemberQ1 July 1st to Sep 30th Oct 1st to Dec 31st Q2 Oct 1st to Dec 31st Jan 1st to March 31st Q3 Jan 1st to March 31st April 1st to June 30th Q4 April 1st to June 30th July 1st to Sep 30th Monthly Reports
Family, Caregiver, Child Demographics
*Required to be updated between 6/1 and 6/30 and 9/1 and 9/30 each yearMONTH OF ENTRY UPDATE OR EXIT DUE DATE IN DATABASE MONTH OF ENTRY UPDATE OR EXIT DUE DATE IN DATABASE July August 10th January February 10th August September 10th February March 10th September October 10th March April 10th October November 10th April May 10th November December 10th May June 10th December January 10th June July 10th Primary Caregiver & Child(ren) Performance Measure Data
Month of Entry, PM Data Due Date in Database Month of Entry, PM Data Due Date in Database July August 10th January February 10th August September 10th February March 10th September October 10th March April 10th October November 10th April May 10th November December 10th May June 10th December January 10th June July 10th Monthly Enrollment Report
Enrollment Month Due Date Enrollment Month Due Date July August 10th-15th January February 10th-15th August September 10th-15th February March 10th-15th September October 10th-15th March April 10th-15th October November 10th-15th April May 10th-15th November December 10th-15th May June 10th-15th December January 10th-15th June July 10th-15th Monthly CQI PDSA
Month Due Date Month Due Date July August 18th January February 18th August September 18th February March 18th September October 18th March April 18th October November 18th April May 18th November December 18th May June 18th December January 18th June July 18th Every Other Month Reports
Staffing Report
Reporting Period Due Date Submisison Month July 1st to Aug 31st Sep 15th Sep Sep 1st to Oct 31st Nov 15th Nov Nov 1st to Dec 31st Jan 15th Jan Jan 1st to Feb 28/29th March 15th March March 1st to April 30th May 15th May May 1st to June 30th July 15th July Quarterly Reports
Quarterly Program Narrative Report
Quarter Reporting Period Due Date First Quarter July 1st – September 30th October 31st Second Quarter October 1st – December 31st January 31st Third Quarter January 1st – March 31st April 30th Fourth Quarter April 1st – June 30th July 31st Quarterly Expenditure Report
Quarter – SFY Reporting Period Due Date First Quarter July 1st – September 30th October 31st Second Quarter October 1st – December 31st January 31st Third Quarter January 1st – March 31st April 30th Fourth Quarter April 1st – June 30th August 15th Twice a Year Reports
Children’s Trust Fund Outcomes Report
Portion of Grant Year Reporting Period Due Date First Half* July 1st – December 30th January 31st Second Half December 31st – June 30th July 31st Yearly Reports
CQI Team Plan
Portion of Grant Year Reporting Period Due Date July to May July to May August 30th Fiscal GL Reconciliation
Portion of Grant Year Reporting Period Due Date July to June July to June September 30th Fiscal Audit
Portion of Grant Year Reporting Period Due Date July to June July to June March 31st As Needed or Required Reports
Staffing Vacancy Report
Month Due Date Month Due Date July As Needed January As Needed August As Needed February As Needed September As Needed March As Needed October As Needed April As Needed November As Needed May As Needed December As Needed June As Needed CQI Summary Report
Portion of Grant Year Reporting Period Due Date July to June July to June Within 30 days of the end of each CQI Project. Grant Renewals
Portion of Grant Year Reporting Period Due Date July to June July to June By no later than April 30th each Year that Renewals are Due. CTF Renewals will be due based on the schedule of CTF Board meetings.
Data System Exports
Input report criteria
(All Values are Required)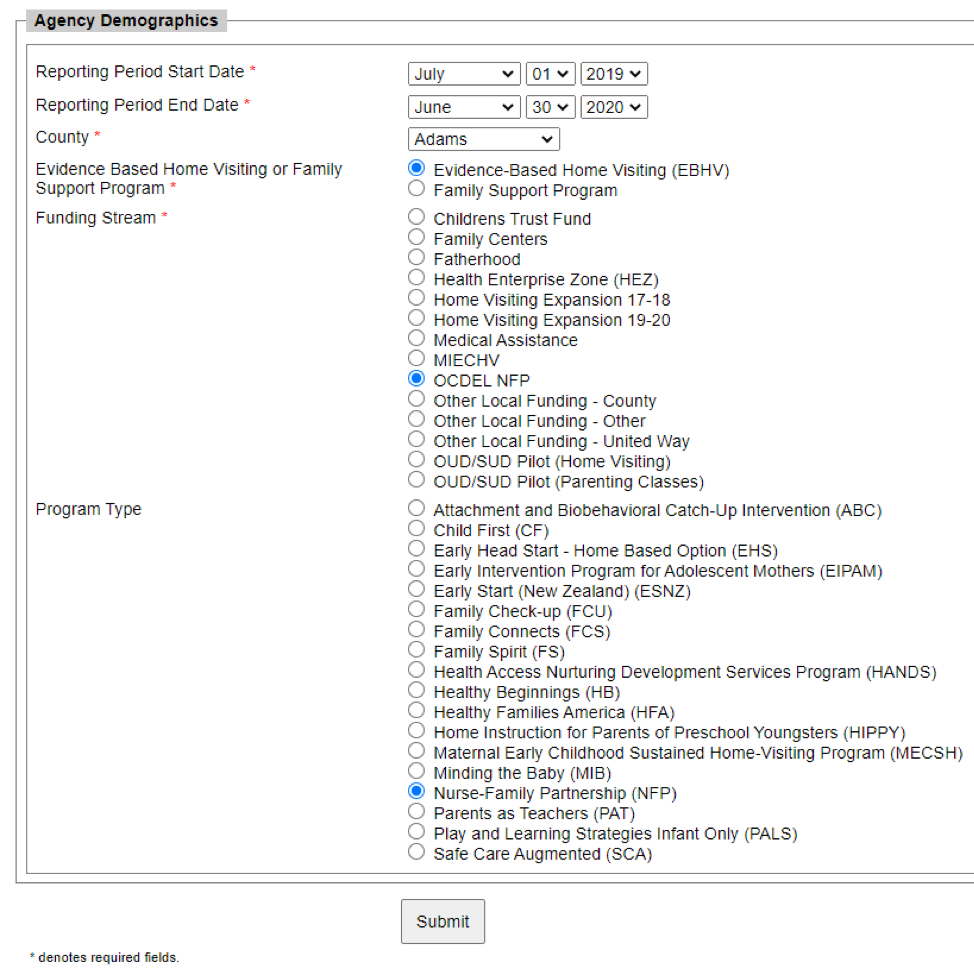
Reporting Period Start Date* &
Reporting Period End Date* County*
EBHV or Family Support Program Model & Funding Stream*
“Submit” to download your chosen Demographics Export

Demographic Export Tables
– Pregnant Under 21
– History of Abuse or Neglect
– History of Substance Abuse
– Substance Abuse Treatment
– Tobacco Use
– Low Student Achievement
– Developmental Delays
– Military
– Disability Benefits